

Resting heart rate, heart rate variability and functional decline in old age
- PMID: 26323697
- PMCID: PMC4610849
- DOI: 10.1503/cmaj.150462
Resting heart rate, heart rate variability and functional decline in old age
Abstract
Background: Heart rate and heart rate variability, markers of cardiac autonomic function, have been linked with cardiovascular disease. We investigated whether heart rate and heart rate variability are associated with functional status in older adults, independent of cardiovascular disease.
Methods: We obtained data from the Prospective Study of Pravastatin in the Elderly at Risk (PROSPER). A total of 5042 participants were included in the present study, and mean follow-up was 3.2 years. Heart rate and heart rate variability were derived from baseline 10-second electrocardiograms. Heart rate variability was defined as the standard deviation of normal-to-normal RR intervals (SDNN). Functional status in basic (ADL) and instrumental (IADL) activities of daily living was measured using Barthel and Lawton scales, at baseline and during follow-up.
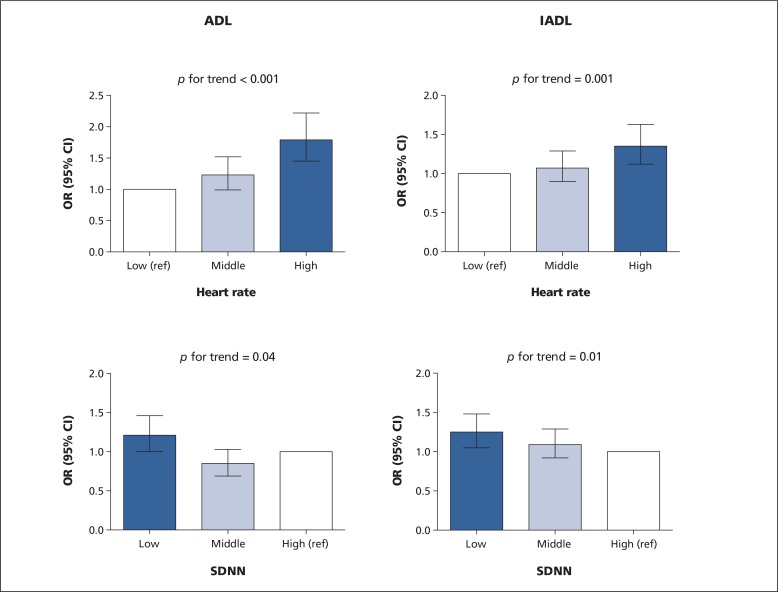
Results: The mean age of the study population was 75.3 years. At baseline, higher heart rate was associated with worse ADL and IADL, and lower SDNN was related to worse IADL (all p values < 0.05). Participants in the highest tertile of heart rate (range 71-117 beats/min) had a 1.79-fold (95% confidence interval [CI] 1.45-2.22) and 1.35-fold (95% CI 1.12-1.63) higher risk of decline in ADL and IADL, respectively (p for trend < 0.001 and 0.001, respectively). Participants in the lowest tertile of SDNN (range 1.70-13.30 ms) had 1.21-fold (95% CI 1.00-1.46) and 1.25-fold (95% CI 1.05-1.48) higher risk of decline in ADL and IADL, respectively (both p for trends < 0.05). All associations were independent of sex, medications, cardiovascular risk factors and comorbidities.
Interpretation: Higher resting heart rate and lower heart rate variability were associated with worse functional status and with higher risk of future functional decline in older adults, independent of cardiovascular disease. This study provides insight into the role of cardiac autonomic function in the development of functional decline.
© 2015 Canadian Medical Association or its licensors.
Figures
References
-
- Fox K, Borer JS, Camm AJ, et al. Resting heart rate in cardiovascular disease. J Am Coll Cardiol 2007;50:823–30. - PubMed
-
- Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J 1996;17:354–81. - PubMed
-
- Palatini P, Benetos A, Julius S. Impact of increased heart rate on clinical outcomes in hypertension: implications for antihypertensive drug therapy. Drugs 2006;66:133–44. - PubMed
-
- Sajadieh A, Nielsen OW, Rasmussen V, et al. Increased heart rate and reduced heart-rate variability are associated with subclinical inflammation in middle-aged and elderly subjects with no apparent heart disease. Eur Heart J 2004;25:363–70. - PubMed
-
- Custodis F, Schirmer SH, Baumhakel M, et al. Vascular pathophysiology in response to increased heart rate. J Am Coll Cardiol 2010;56:1973–83. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources