

Health sector employment: a tracer indicator for universal health coverage in national Social Protection Floors
- PMID: 26323724
- PMCID: PMC4556411
- DOI: 10.1186/s12960-015-0056-9
Health sector employment: a tracer indicator for universal health coverage in national Social Protection Floors
Abstract
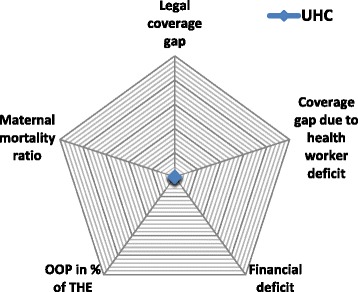
Background: Health sector employment is a prerequisite for availability, accessibility, acceptability and quality (AAAQ) of health services. Thus, in this article health worker shortages are used as a tracer indicator estimating the proportion of the population lacking access to such services: The SAD (ILO Staff Access Deficit Indicator) estimates gaps towards UHC in the context of Social Protection Floors (SPFs). Further, it highlights the impact of investments in health sector employment equity and sustainable development.
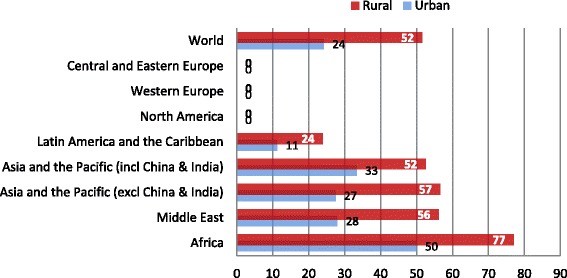
Methods: The SAD is used to estimate the share of the population lacking access to health services due to gaps in the number of skilled health workers. It is based on the difference of the density of the skilled health workforce per population in a given country and a threshold indicating UHC staffing requirements. It identifies deficits, differences and developments in access at global, regional and national levels and between rural and urban areas.
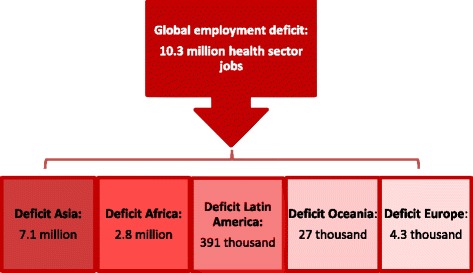
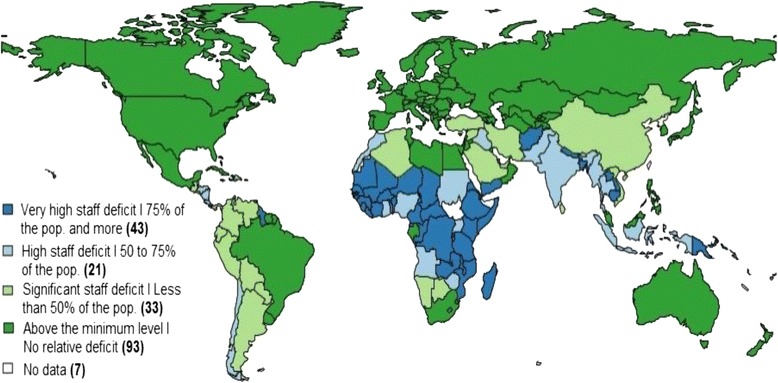
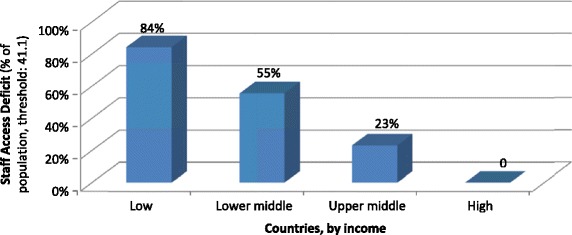
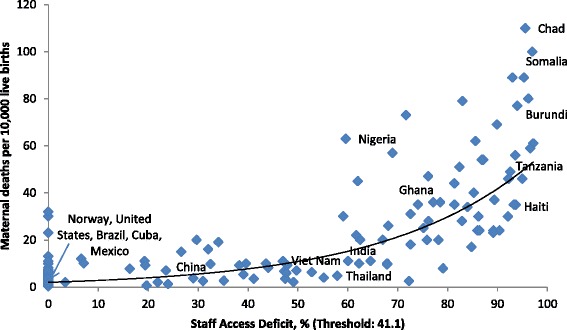
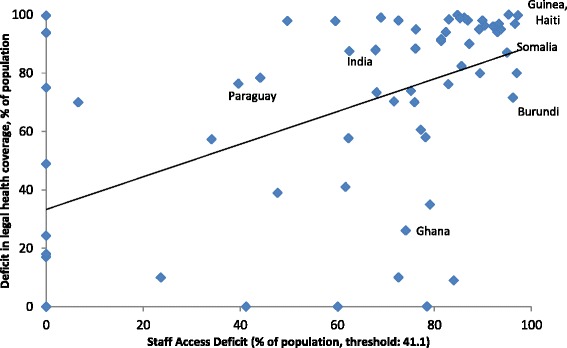
Results: In 2014, the global UHC deficit in numbers of health workers is estimated at 10.3 million, with most important gaps in Asia (7.1 million) and Africa (2.8 million). Globally, 97 countries are understaffed with significantly higher gaps in rural than in urban areas. Most affected are low-income countries, where 84 per cent of the population remains excluded from access due to the lack of skilled health workers. A positive correlation of health worker employment and population health outcomes could be identified. Legislation is found to be a prerequisite for closing access as gaps.
Conclusions: Health worker shortages hamper the achievement of UHC and aggravate weaknesses of health systems. They have major impacts on socio-economic development, particularly in the world's poorest countries where they act as drivers of health inequities. Closing the gaps by establishing inclusive multi-sectoral policy approaches based on the right to health would significantly increase equity, reduce poverty due to ill health and ultimately contribute to sustainable development and social justice.
Figures
References
-
- Global Health Workforce Alliance and World Health Organization . A universal truth: no health without a workforce. Geneva: Third Global Forum on Human Resources for Health Report; 2013.
-
- Scheil-Adlung X, Bonnet F, Wiechers T, Ayanbayi T. New approaches to measuring deficits in social health protection coverage in vulnerable countries, World Health Report. 2010. Background paper 56. http://www.who.int/healthsystems/topics/financing/healthreport/BP56Measu.... Accessed 21 May 2015.
-
- ILO. R 202 – social protection floors recommendation, 2012 (No. 202). Geneva: 101st ILC session; 2012. http://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_INS... Accessed 13 January 2015.
-
- WHO. Global Health Workforce Statistics database. Geneva: World Health Organization. http://www.who.int/hrh/statistics/hwfstats/. Accessed 16 January 2015
-
- ILO . World Social Protection Report 2014/15: building economic recovery, inclusive development and social justice. Geneva: International Labour Organization; 2014.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
