

4.7-T diffusion tensor imaging of acute traumatic peripheral nerve injury
- PMID: 26323827
- PMCID: PMC4786003
- DOI: 10.3171/2015.6.FOCUS1590
4.7-T diffusion tensor imaging of acute traumatic peripheral nerve injury
Abstract
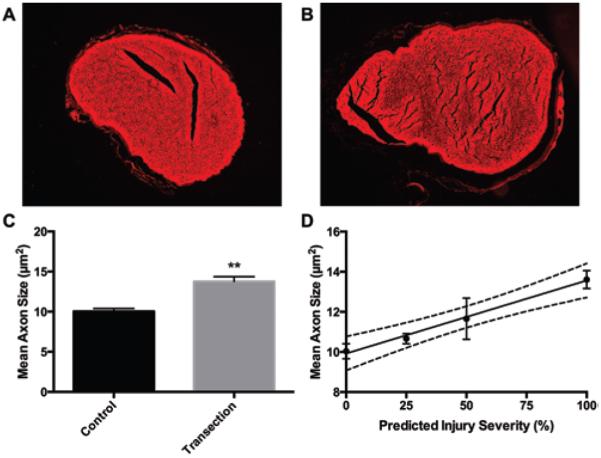
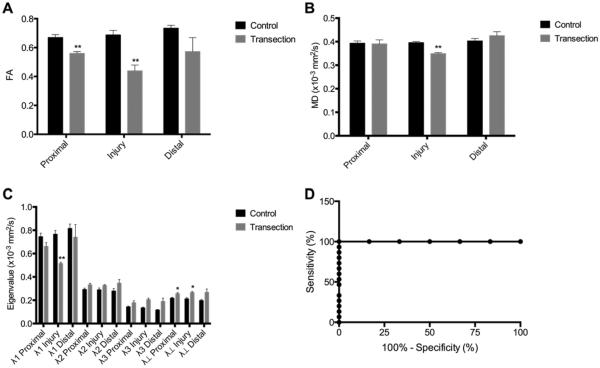
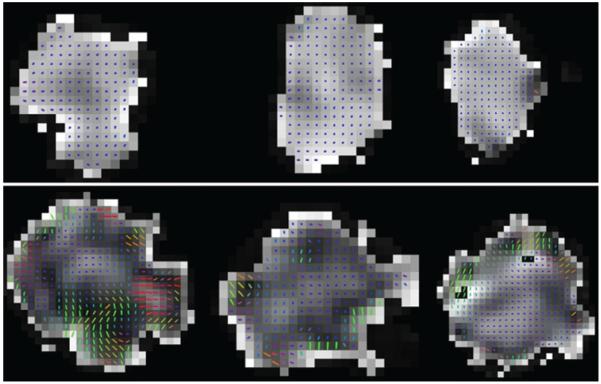
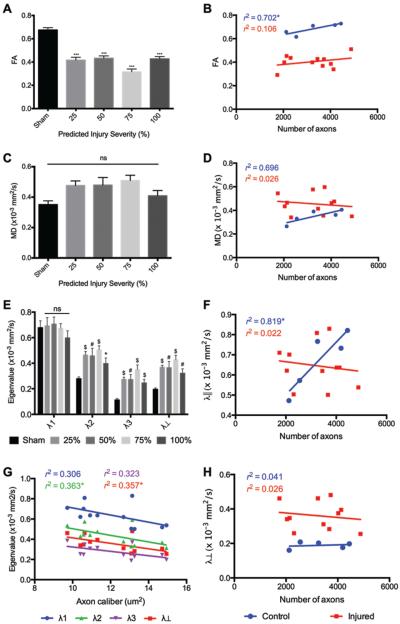
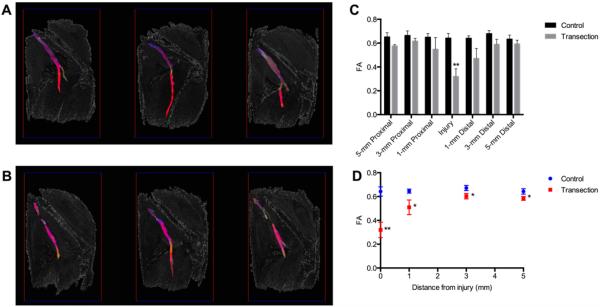
Diagnosis and management of peripheral nerve injury is complicated by the inability to assess microstructural features of injured nerve fibers via clinical examination and electrophysiology. Diffusion tensor imaging (DTI) has been shown to accurately detect nerve injury and regeneration in crush models of peripheral nerve injury, but no prior studies have been conducted on nerve transection, a surgical emergency that can lead to permanent weakness or paralysis. Acute sciatic nerve injuries were performed microsurgically to produce multiple grades of nerve transection in rats that were harvested 1 hour after surgery. High-resolution diffusion tensor images from ex vivo sciatic nerves were obtained using diffusion-weighted spin-echo acquisitions at 4.7 T. Fractional anisotropy was significantly reduced at the injury sites of transected rats compared with sham rats. Additionally, minor eigenvalues and radial diffusivity were profoundly elevated at all injury sites and were negatively correlated to the degree of injury. Diffusion tensor tractography showed discontinuities at all injury sites and significantly reduced continuous tract counts. These findings demonstrate that high-resolution DTI is a promising tool for acute diagnosis and grading of traumatic peripheral nerve injuries.
Keywords: AUC = area under the curve; DTI = diffusion tensor imaging; DTPA = diethylene triamine pentaacetic acid; FA = fractional anisotropy; MD = mean diffusivity; MRI; MRN = MR neurography; PBS = phosphate-buffered saline; PFA = paraformaldehyde; ROC = receiver-operator characteristic; ROI = region of interest; SNR = signal-to-noise ratio; diffusion tensor imaging; diffusion tensor tractography; nerve transection; neurography; neurotmesis; peripheral nerve injury; λ‖ = axial diffusivity; λ⊥ = radial diffusivity.
Figures

References
-
- Aagaard BD, Lazar DA, Lankerovich L, Andrus K, Hayes CE, Maravilla K, et al. High-resolution magnetic resonance imaging is a noninvasive method of observing injury and recovery in the peripheral nervous system. Neurosurgery. 2003;53:199–204. - PubMed
-
- Agosta F, Absinta M, Sormani MP, Ghezzi A, Bertolotto A, Montanari E, et al. In vivo assessment of cervical cord damage in MS patients: a longitudinal diffusion tensor MRI study. Brain. 2007;130:2211–2219. - PubMed
-
- Bain JR, Mackinnon SE, Hunter DA. Functional evaluation of complete sciatic, peroneal, and posterior tibial nerve lesions in the rat. Plast Reconstr Surg. 1989;83:129–138. - PubMed
-
- Beaulieu C, Does MD, Snyder RE, Allen PS. Changes in water diffusion due to Wallerian degeneration in peripheral nerve. Magn Reson Med. 1996;36:627–631. - PubMed
-
- Behr B, Schnabel R, Mirastschijski U, Ibrahim B, Angenstein F, Schneider W. Magnetic resonance imaging monitoring of peripheral nerve regeneration following neurotmesis at 4.7 Tesla. Plast Reconstr Surg. 2009;123:1778–1788. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
