

Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure
- PMID: 26323938
- PMCID: PMC4779593
- DOI: 10.1056/NEJMoa1506459
Adaptive Servo-Ventilation for Central Sleep Apnea in Systolic Heart Failure
Abstract
Background: Central sleep apnea is associated with poor prognosis and death in patients with heart failure. Adaptive servo-ventilation is a therapy that uses a noninvasive ventilator to treat central sleep apnea by delivering servo-controlled inspiratory pressure support on top of expiratory positive airway pressure. We investigated the effects of adaptive servo-ventilation in patients who had heart failure with reduced ejection fraction and predominantly central sleep apnea.
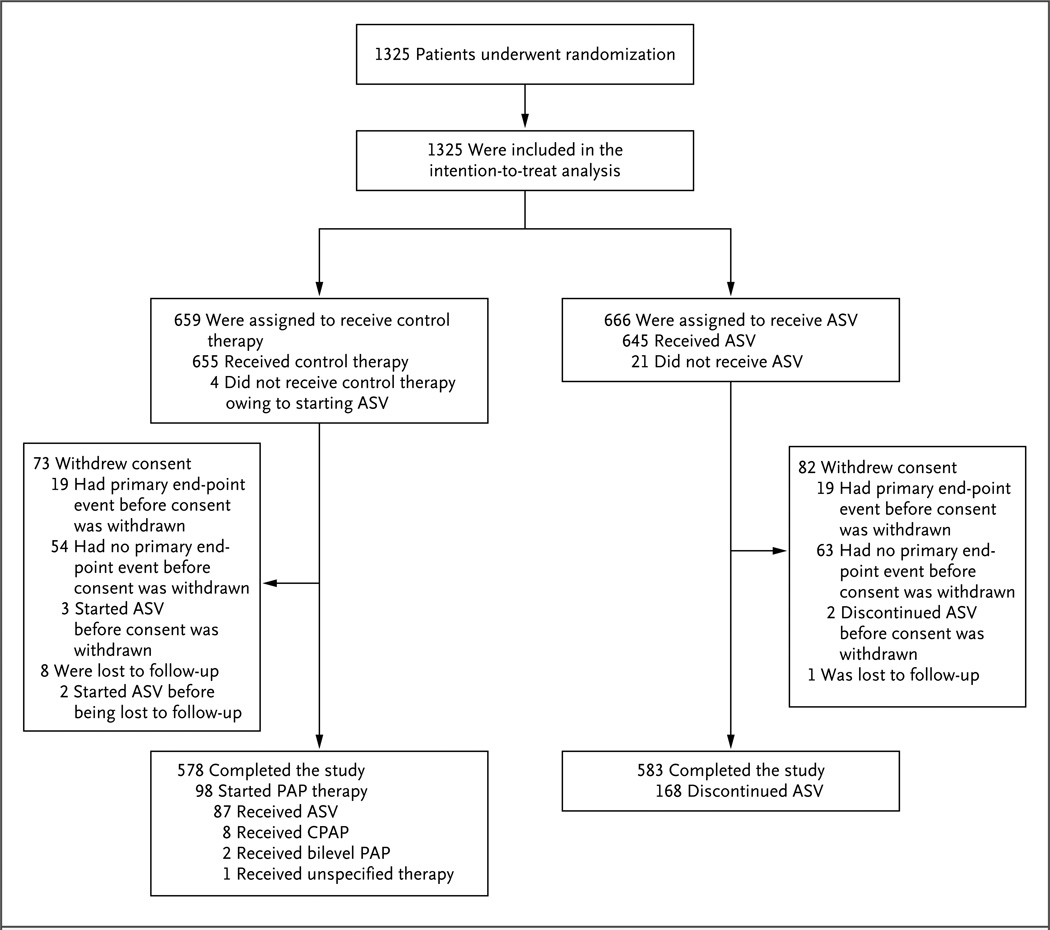
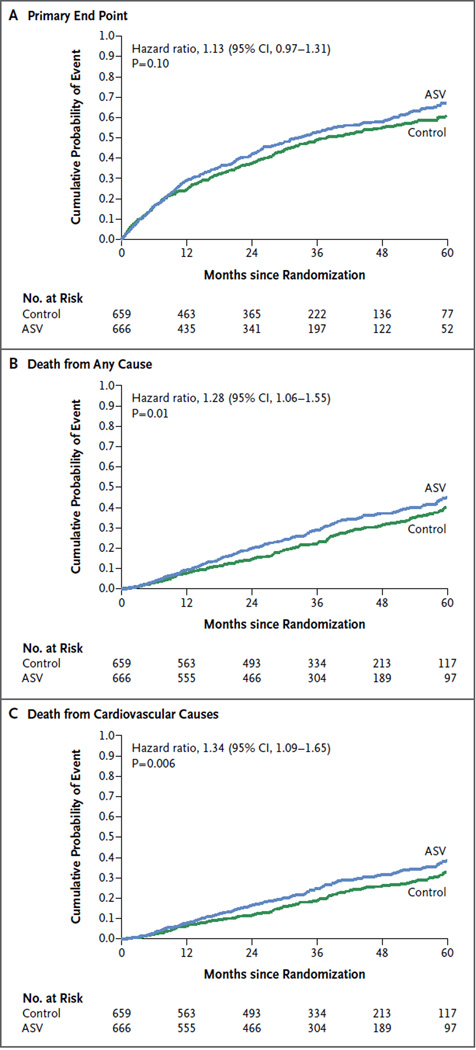
Methods: We randomly assigned 1325 patients with a left ventricular ejection fraction of 45% or less, an apnea-hypopnea index (AHI) of 15 or more events (occurrences of apnea or hypopnea) per hour, and a predominance of central events to receive guideline-based medical treatment with adaptive servo-ventilation or guideline-based medical treatment alone (control). The primary end point in the time-to-event analysis was the first event of death from any cause, lifesaving cardiovascular intervention (cardiac transplantation, implantation of a ventricular assist device, resuscitation after sudden cardiac arrest, or appropriate lifesaving shock), or unplanned hospitalization for worsening heart failure.
Results: In the adaptive servo-ventilation group, the mean AHI at 12 months was 6.6 events per hour. The incidence of the primary end point did not differ significantly between the adaptive servo-ventilation group and the control group (54.1% and 50.8%, respectively; hazard ratio, 1.13; 95% confidence interval [CI], 0.97 to 1.31; P=0.10). All-cause mortality and cardiovascular mortality were significantly higher in the adaptive servo-ventilation group than in the control group (hazard ratio for death from any cause, 1.28; 95% CI, 1.06 to 1.55; P=0.01; and hazard ratio for cardiovascular death, 1.34; 95% CI, 1.09 to 1.65; P=0.006).
Conclusions: Adaptive servo-ventilation had no significant effect on the primary end point in patients who had heart failure with reduced ejection fraction and predominantly central sleep apnea, but all-cause and cardiovascular mortality were both increased with this therapy. (Funded by ResMed and others; SERVE-HF ClinicalTrials.gov number, NCT00733343.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Heart Failure and Sleep-Disordered Breathing--The Plot Thickens.N Engl J Med. 2015 Sep 17;373(12):1166-7. doi: 10.1056/NEJMe1510397. Epub 2015 Sep 1. N Engl J Med. 2015. PMID: 26323939 No abstract available.
-
Heart failure: Central sleep apnoea in HF--what can we learn from SERVE-HF?Nat Rev Cardiol. 2015 Dec;12(12):686-7. doi: 10.1038/nrcardio.2015.168. Epub 2015 Nov 3. Nat Rev Cardiol. 2015. PMID: 26525541 No abstract available.
-
Adaptive Servo-ventilation and the Treatment of Central Sleep Apnea in Heart Failure. Let's Not Throw the Baby Out with the Bathwater.Am J Respir Crit Care Med. 2016 Feb 15;193(4):357-9. doi: 10.1164/rccm.201511-2198ED. Am J Respir Crit Care Med. 2016. PMID: 26646208 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):690-1. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886528 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):687-8. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886529 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):688. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886530 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):688. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886531 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):689. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886532 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):689. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886533 No abstract available.
-
Adaptive Servo-Ventilation for Central Sleep Apnea in Heart Failure.N Engl J Med. 2016 Feb 18;374(7):689-90. doi: 10.1056/NEJMc1515007. N Engl J Med. 2016. PMID: 26886534 No abstract available.
-
Adaptive Servo-Ventilation and Central Apnea Associated with Systolic Heart Failure.J Clin Sleep Med. 2016 Jan;12(1):147-50. doi: 10.5664/jcsm.5420. J Clin Sleep Med. 2016. PMID: 26888594 Free PMC article. No abstract available.
-
Noninvasive Ventilation and Clinical Outcome.Am J Respir Crit Care Med. 2016 Aug 15;194(4):510-3. doi: 10.1164/rccm.201602-0411RR. Am J Respir Crit Care Med. 2016. PMID: 27267940 No abstract available.
-
Withdrawing ASV therapy in clinical practice: trials and tribulations.Sleep Med. 2017 Sep;37:208-209. doi: 10.1016/j.sleep.2017.03.001. Epub 2017 Mar 9. Sleep Med. 2017. PMID: 28366779 No abstract available.
References
-
- Oldenburg O, Lamp B, Faber L, Teschler H, Horstkotte D, Töpfer V. Sleep-disordered breathing in patients with symptomatic heart failure: a contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail. 2007;9:251–257. - PubMed
-
- Lévy P, Pépin J-L, Tamisier R, Neuder Y, Baguet J-P, Javaheri S. Prevalence and impact of central sleep apnea in heart failure. Sleep Med Clin. 2007;2:615–621.
-
- Oldenburg O, Bitter T, Wiemer M, Langer C, Horstkotte D, Piper C. Pulmonary capillary wedge pressure and pulmonary arterial pressure in heart failure patients with sleep-disordered breathing. Sleep Med. 2009;10:726–730. - PubMed
-
- Bitter T, Westerheide N, Prinz C, et al. Cheyne-Stokes respiration and obstructive sleep apnoea are independent risk factors for malignant ventricular arrhythmias requiring appropriate cardioverter-defibrillator therapies in patients with congestive heart failure. Eur Heart J. 2011;32:61–74. - PubMed
-
- Kasai T, Floras JS, Bradley TD. Sleep apnea and cardiovascular disease: a bidirectional relationship. Circulation. 2012;126:1495–1510. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous