

Intermediate and Longer-Term Outcomes From a Prospective Active-Surveillance Program for Favorable-Risk Prostate Cancer
- PMID: 26324359
- PMCID: PMC4863946
- DOI: 10.1200/JCO.2015.62.5764
Intermediate and Longer-Term Outcomes From a Prospective Active-Surveillance Program for Favorable-Risk Prostate Cancer
Abstract
Purpose: To assess long-term outcomes of men with favorable-risk prostate cancer in a prospective, active-surveillance program.
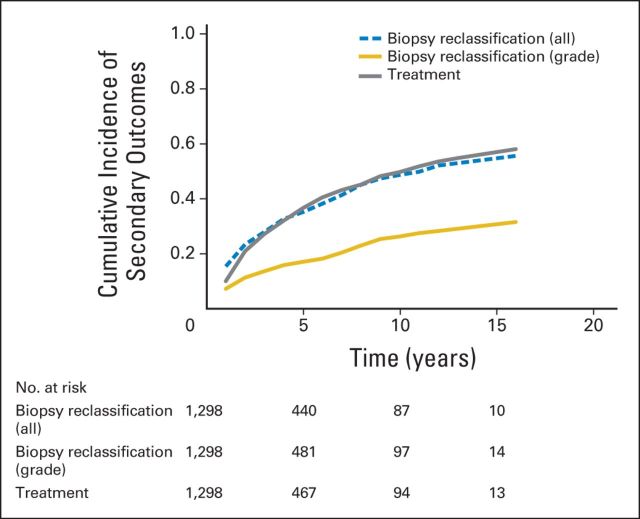
Methods: Curative intervention was recommended for disease reclassification to higher cancer grade or volume on prostate biopsy. Primary outcomes were overall, cancer-specific, and metastasis-free survival. Secondary outcomes were the cumulative incidence of reclassification and curative intervention. Factors associated with grade reclassification and curative intervention were evaluated in a Cox proportional hazards model.
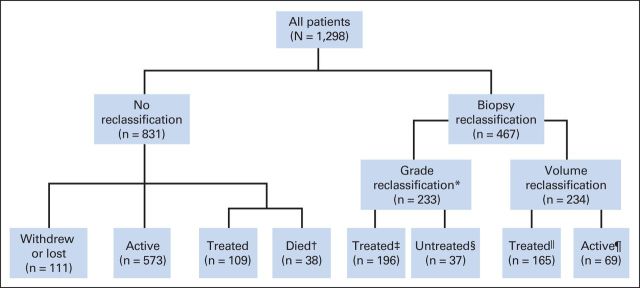
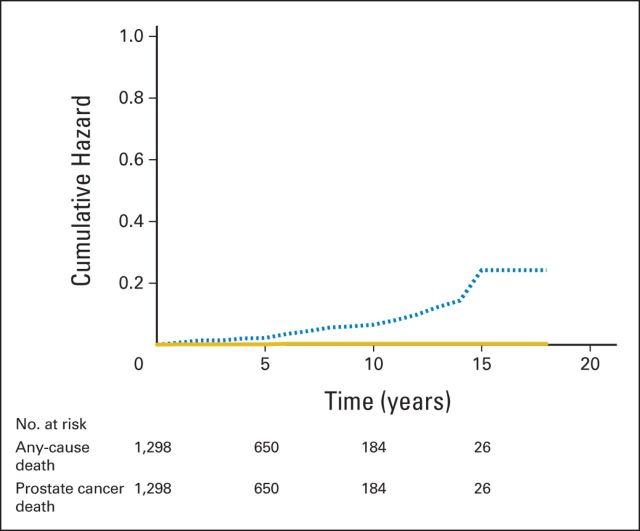
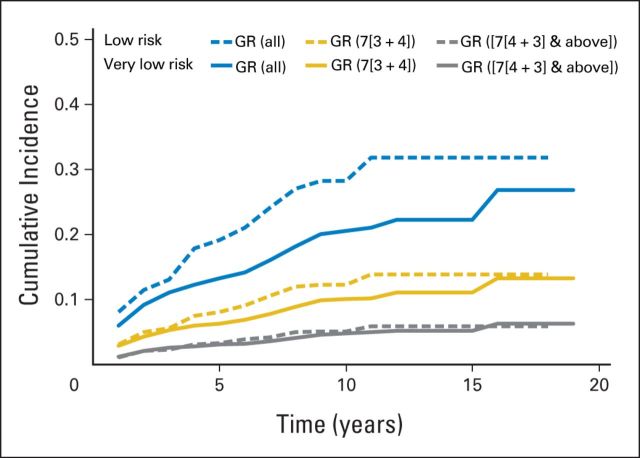
Results: A total of 1,298 men (median age, 66 years) with a median follow-up of 5 years (range, 0.01 to 18.00 years) contributed 6,766 person-years of follow-up since 1995. Overall, cancer-specific, and metastasis-free survival rates were 93%, 99.9%, and 99.4%, respectively, at 10 years and 69%, 99.9%, and 99.4%, respectively, at 15 years. The cumulative incidence of grade reclassification was 26% at 10 years and was 31% at 15 years; cumulative incidence of curative intervention was 50% at 10 years and was 57% at 15 years. The median treatment-free survival was 8.5 years (range, 0.01 to 18 years). Factors associated with grade reclassification were older age (hazard ratio [HR], 1.03 for each additional year; 95% CI, 1.01 to 1.06), prostate-specific antigen density (HR, 1.21 per 0.1 unit increase; 95% CI, 1.12 to 1.46), and greater number of positive biopsy cores (HR, 1.47 for each additional positive core; 95% CI, 1.26 to 1.69). Factors associated with intervention were prostate-specific antigen density (HR, 1.38 per 0.1 unit increase; 95% CI, 1.22 to 1.56) and a greater number of positive biopsy cores (HR, 1.35 for one additional positive core; 95% CI, 1.19 to 1.53).
Conclusion: Men with favorable-risk prostate cancer should be informed of the low likelihood of harm from their diagnosis and should be encouraged to consider surveillance rather than curative intervention.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Comment in
-
Personalizing the Use of Active Surveillance As an Initial Approach for Men With Newly Diagnosed Prostate Cancer.J Clin Oncol. 2015 Oct 20;33(30):3365-6. doi: 10.1200/JCO.2015.63.6118. Epub 2015 Aug 31. J Clin Oncol. 2015. PMID: 26324374 No abstract available.
-
Prostate cancer: AS--contemplation, not intervention.Nat Rev Urol. 2015 Nov;12(11):595. doi: 10.1038/nrurol.2015.224. Epub 2015 Sep 15. Nat Rev Urol. 2015. PMID: 26369726 No abstract available.
-
Prostate cancer: AS-contemplation, not intervention.Nat Rev Clin Oncol. 2015 Nov;12(11):623. doi: 10.1038/nrclinonc.2015.160. Epub 2015 Sep 15. Nat Rev Clin Oncol. 2015. PMID: 26370606 No abstract available.
-
Reply to M.C. Scholz et al.J Clin Oncol. 2016 Apr 10;34(11):1284. doi: 10.1200/JCO.2015.65.9755. Epub 2016 Feb 16. J Clin Oncol. 2016. PMID: 26884568 No abstract available.
-
Reply to M.C. Scholz et al.J Clin Oncol. 2016 Apr 10;34(11):1284. doi: 10.1200/JCO.2015.65.9763. Epub 2016 Feb 16. J Clin Oncol. 2016. PMID: 26884570 No abstract available.
-
Query About the Frequency of Biopsy Complications.J Clin Oncol. 2016 Apr 10;34(11):1284. doi: 10.1200/JCO.2015.65.6827. Epub 2016 Feb 16. J Clin Oncol. 2016. PMID: 26884576 No abstract available.
-
Intermediate and longer-term outcomes from a prospective active-surveillance program for favorable-risk prostate cancer. Tosoian JJ, Mamawala M, Epstein JI, Landis P, Wolf S, Trock BJ, Carter HB.J Clin Oncol. 2015 Oct 20;33(30):3379-85. [Epub 2015 Aug 31]. doi: 10.1200/JCO.2015.62.5764.Urol Oncol. 2017 Mar;35(3):121-122. doi: 10.1016/j.urolonc.2016.12.019. Epub 2017 Feb 1. Urol Oncol. 2017. PMID: 28159497
References
-
- Albertsen PC, Hanley JA, Fine J. 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA. 2005;293:2095–2101. - PubMed
-
- Moyer VA Force USPST. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157:120–134. - PubMed
-
- Hayes JH, Barry MJ. Screening for prostate cancer with the prostate-specific antigen test: A review of current evidence. JAMA. 2014;311:1143–1149. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
