

Clinical predictors of antibiotic prescribing for acutely ill children in primary care: an observational study
- PMID: 26324495
- PMCID: PMC4540398
- DOI: 10.3399/bjgp15X686497
Clinical predictors of antibiotic prescribing for acutely ill children in primary care: an observational study
Abstract
Background: Antibiotic overuse and inappropriate prescribing drive antibiotic resistance. Children account for a high proportion of antibiotics prescribed in primary care.
Aim: To determine the predictors of antibiotic prescription in young children presenting to UK general practices with acute illness.
Design and setting: Prospective observational study in general practices in Wales.
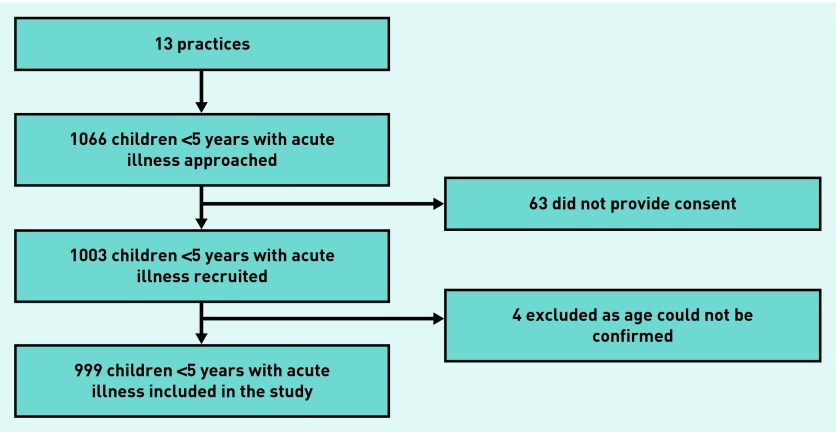
Method: A total of 999 children were recruited from 13 practices between March 2008 and July 2010. Multilevel, multivariable logistic regression analysis was performed to determine predictors of antibiotic prescribing.
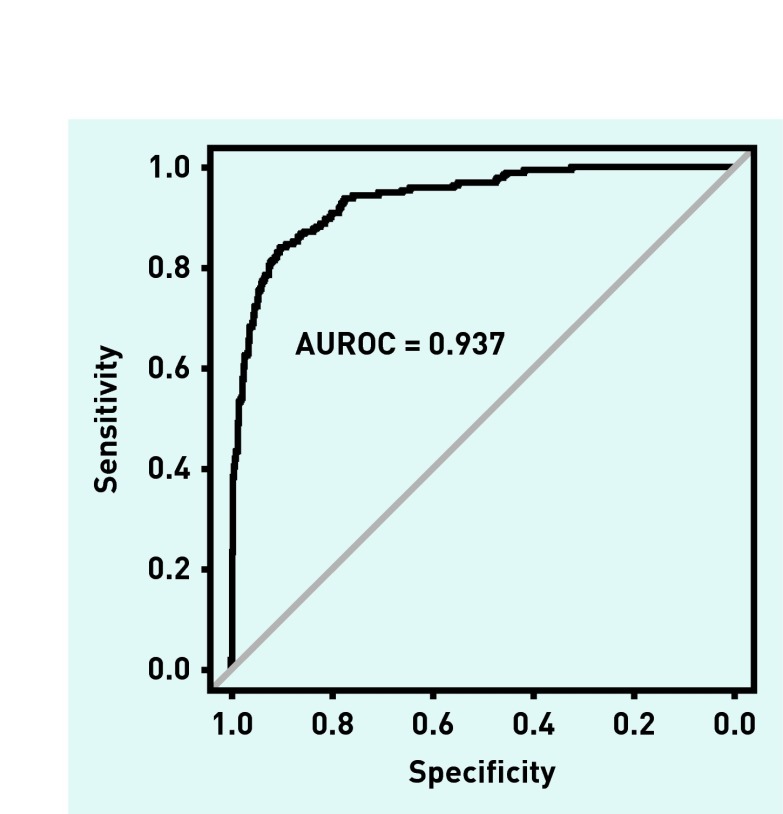
Results: Oral antibiotics were prescribed to 261 children (26.1%). Respiratory infections were responsible for 77.4% of antibiotic prescriptions. The multivariable model included 719 children. Children were more likely to be prescribed antibiotics if they were older (odds ratio [OR] 1.3; 95% confidence intervals [CI] = 1.1 to 1.7); presented with poor sleep (OR 2.7; 95% CI = 1.5 to 5.0); had abnormal ear (OR 6.5; 95% CI = 2.5 to 17.2), throat (OR 2.2; 95% CI = 1.1 to 4.5) or chest examination (OR 13.6; 95% CI = 5.8 to 32.2); were diagnosed with lower respiratory tract infection (OR 9.5; 95% CI = 3.7 to 25.5), tonsillitis/sore throat (OR 119.3; 95% CI = 28.2 to 504.6), ear infection (OR 26.5; 95% CI = 7.4 to 95.7) or urinary tract infection (OR 12.7; 95% CI = 4.4 to 36.5); or if the responsible clinician perceived the child to be moderately to severely unwell (OR 4.0; 95% CI = 1.4 to 11.4). The area under the receiver operating characteristic curve was 0.9371.
Conclusion: Respiratory infections were responsible for 74.4% of antibiotic prescriptions. Diagnoses of tonsillitis, sore throat, or ear infection were associated most with antibiotic prescribing. Diagnosis seemed to be more important than abnormal examination findings in predicting antibiotic prescribing, although these were correlated.
Keywords: acute disease; antibacterial agents; antibiotic prescribing; children; infection; primary care.
© British Journal of General Practice 2015.
Figures
References
-
- Department of Health . UK five year antimicrobial resistance strategy 2013 to 2018. London: The Stationery Office; 2013.
-
- World Health Organization Antimicrobial resistance: global report on surveillance. 2014 http://www.who.int/drugresistance/documents/surveillancereport/en/ (accessed 26 Jun 2015)
-
- Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096. - PubMed
-
- Goossens H, Ferech M, Vander Stichele R, et al. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365:579–587. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical