

Clinical and Translational Results of a Phase II, Randomized Trial of an Anti-IGF-1R (Cixutumumab) in Women with Breast Cancer That Progressed on Endocrine Therapy
- PMID: 26324738
- PMCID: PMC5548297
- DOI: 10.1158/1078-0432.CCR-15-0588
Clinical and Translational Results of a Phase II, Randomized Trial of an Anti-IGF-1R (Cixutumumab) in Women with Breast Cancer That Progressed on Endocrine Therapy
Abstract
Purpose: This phase II trial evaluated the efficacy and safety of cixutumumab, a human anti-insulin-like growth factor receptor 1 (IGF-1R) monoclonal IgG1 antibody, and explored potential biomarkers in postmenopausal women with hormone receptor-positive breast cancer.
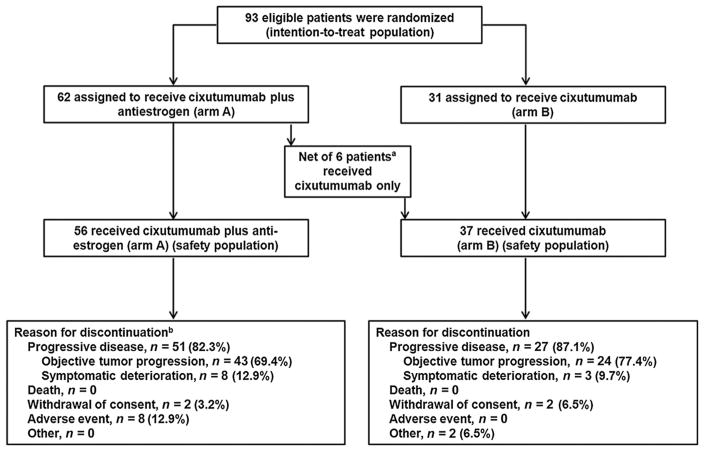
Experimental design: Patients with hormone receptor-positive breast cancer that progressed on antiestrogen therapy received (2:1 randomization) cixutumumab 10 mg/kg and the same antiestrogen (arm A) or cixutumumab alone (arm B) every 2 weeks (q2w). Primary endpoint was progression-free survival (PFS); secondary endpoints included overall survival (OS) and safety. Correlative analyses of IGF-1R, total insulin receptor (IR), and IR isoforms A (IR-A) and B (IR-B) expression in tumor tissue were explored.
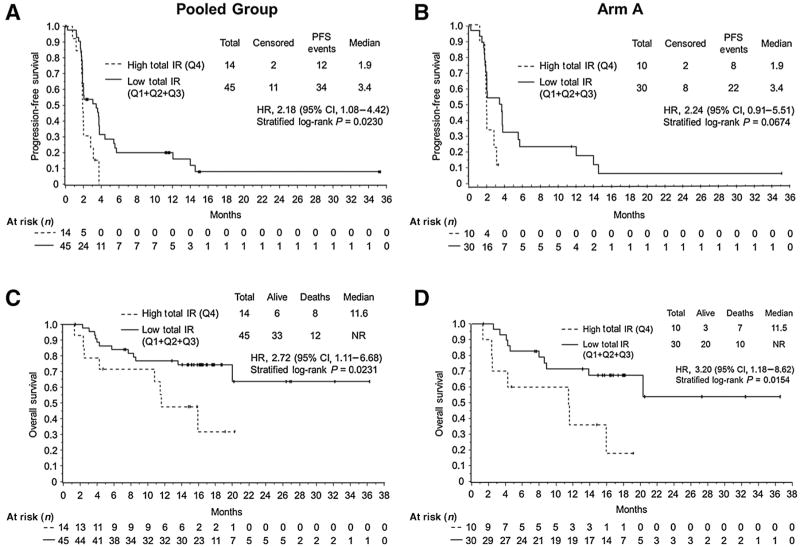
Results: Ninety-three patients were randomized (arm A, n = 62; arm B, n = 31). Median PFS was 2.0 and 3.1 months for arm A and arm B, respectively. Secondary efficacy measures were similar between the arms. Overall, cixutumumab was well tolerated. IGF-1R expression was not associated with clinical outcomes. Regardless of the treatment, lower IR-A, IR-B, and total IR mRNA expression in tumor tissue was significantly associated with longer PFS [IR-A: HR, 2.62 (P = 0.0062); IR-B: HR, 2.21 (P = 0.0202); and total IR: HR, 2.18 (P = 0.0230)] and OS [IR-A: HR, 2.94 (P = 0.0156); IR-B: HR, 2.69 (P = 0.0245); and total IR: HR, 2.72 (P = 0.0231)].
Conclusions: Cixutumumab (10 mg/kg) with or without antiestrogen q2w had an acceptable safety profile, but no significant clinical efficacy. Patients with low total IR, IR-A, and IR-B mRNA expression levels had significantly longer PFS and OS, independent of the treatment. The prognostic or predictive value of IR as a biomarker for IGF-1R-targeted therapies requires further validation.
©2015 American Association for Cancer Research.
Conflict of interest statement
P. Haluska reports receiving speakers bureau honoraria from Boehringer Ingleheim, is a consultant/advisory board member for Boehringer Ingleheim, Bristol-Myers Squibb, and Medimmune, and reports receiving commercial research support from Bristol-Myers Squibb, ImClone, and Medimmune. No potential conflicts of interest were disclosed by the other authors.
Figures

References
-
- Ciruelos Gil EM. Targeting the PI3K/AKT/mTOR pathway in estrogen receptor-positive breast cancer. Cancer Treat Rev. 2014;40:862–71. - PubMed
-
- Santen RJ, Song RX, Zhang Z, Yue W, Kumar R. Adaptive hypersensitivity to estrogen: mechanism for sequential responses to hormonal therapy in breast cancer. Clin Cancer Res. 2004;10:337S–45S. - PubMed
-
- Song RX, Zhang Z, Chen Y, Bao Y, Santen RJ. Estrogen signaling via a linear pathway involving insulin-like growth factor I receptor, matrix metalloproteinases, and epidermal growth factor receptor to activate mitogen-activated protein kinase in MCF-7 breast cancer cells. Endocrinology. 2007;148:4091–101. - PMC - PubMed
-
- Knowlden JM, Hutcheson IR, Barrow D, Gee JM, Nicholson RI. Insulin-like growth factor-I receptor signaling in tamoxifen-resistant breast cancer: a supporting role to the epidermal growth factor receptor. Endocrinology. 2005;146:4609–18. - PubMed
-
- Chong K, Subramanian A, Sharma A, Mokbel K. Measuring IGF-1, ER-α and EGFR expression can predict tamoxifen-resistance in ER-positive breast cancer. Anticancer Res. 2011;31:23–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
