

Influence of N-acetylcysteine on chronic bronchitis or COPD exacerbations: a meta-analysis
- PMID: 26324807
- PMCID: PMC9487680
- DOI: 10.1183/16000617.00002215
Influence of N-acetylcysteine on chronic bronchitis or COPD exacerbations: a meta-analysis
Abstract
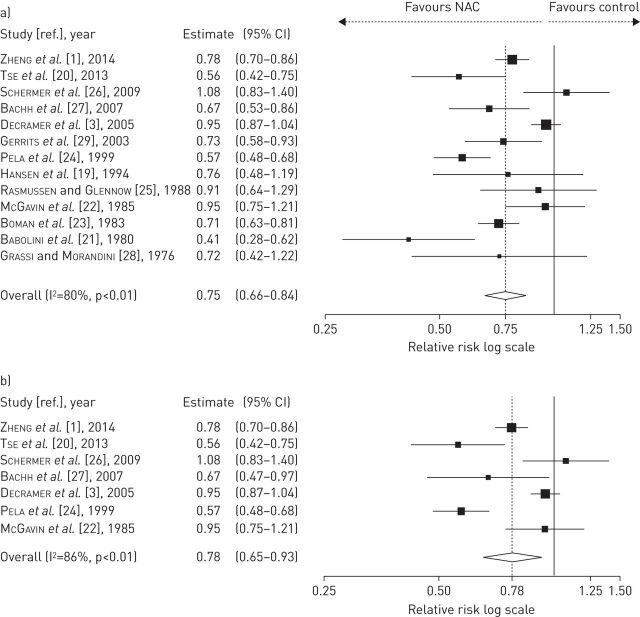
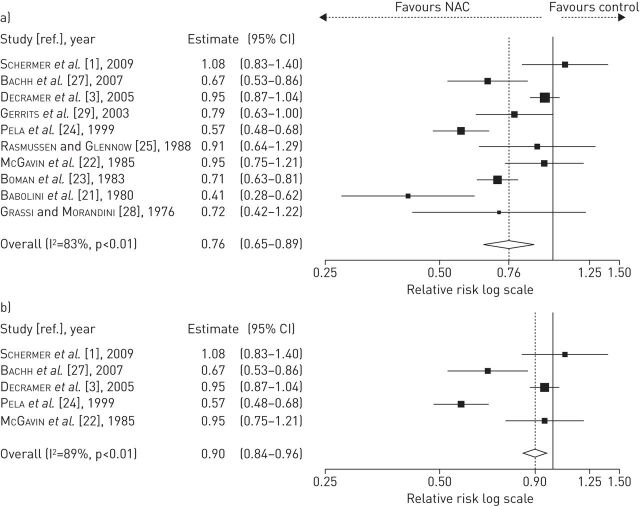
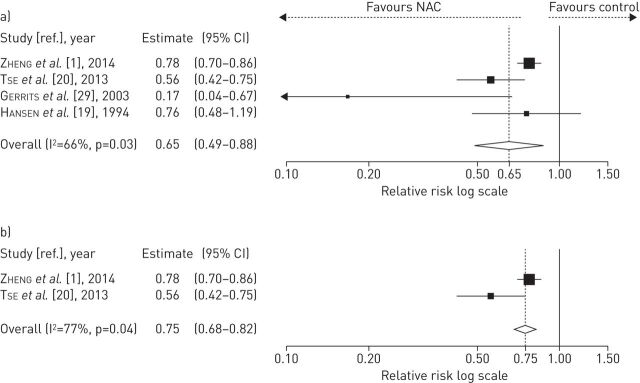
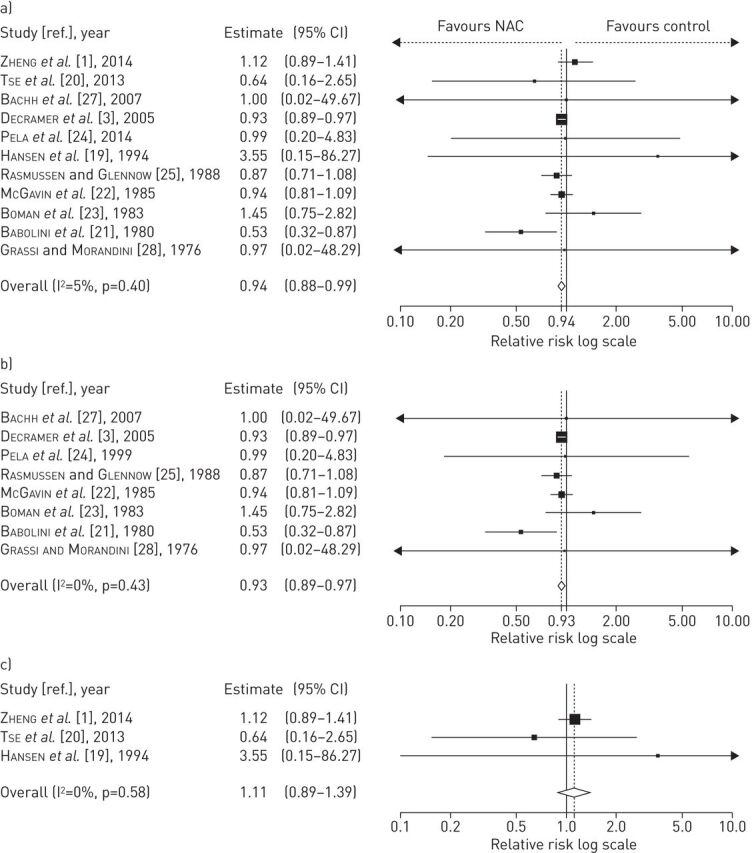
In order to clarify the possible role of N-acetylcysteine (NAC) in the treatment of patients with chronic bronchitis and chronic obstructive pulmonary disease (COPD), we have carried out a meta-analysis testing the available evidence that NAC treatment may be effective in preventing exacerbations of chronic bronchitis or COPD and evaluating whether there is a substantial difference between the responses induced by low (≤ 600 mg per day) and high (> 600 mg per day) doses of NAC. The results of the present meta-analysis (13 studies, 4155 COPD patients, NAC n = 1933; placebo or controls n = 2222) showed that patients treated with NAC had significantly and consistently fewer exacerbations of chronic bronchitis or COPD (relative risk 0.75, 95% CI 0.66-0.84; p < 0.01), although this protective effect was more apparent in patients without evidence of airway obstruction. However, high doses of NAC were also effective in patients suffering from COPD diagnosed using spirometric criteria (relative risk 0.75, 95% CI 0.68-0.82; p = 0.04). NAC was well tolerated and the risk of adverse reactions was not dose-dependent (low doses relative risk 0.93, 95% CI 0.89-0.97; p = 0.40; high doses relative risk 1.11, 95% CI 0.89-1.39; p = 0.58). The strong signal that comes from this meta-analysis leads us to state that if a patient suffering from chronic bronchitis presents a documented airway obstruction, NAC should be administered at a dose of ≥ 1200 mg per day to prevent exacerbations, while if a patient suffers from chronic bronchitis, but is without airway obstruction, a regular treatment of 600 mg per day seems to be sufficient.
Copyright ©ERS 2015.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside the online version of this article at
Figures

References
-
- Zheng JP, Wen FQ, Bai CX, et al. Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respir Med 2014; 2: 187–194. - PubMed
-
- Cazzola M, Matera MG. N-acetylcysteine in COPD may be beneficial, but for whom? Lancet Respir Med 2014; 2: 166–167. - PubMed
-
- Decramer M, Rutten-van Mölken M, Dekhuijzen PN, et al. Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (Bronchitis Randomized on NAC Cost–Utility Study, BRONCUS): a randomised placebo-controlled trial. Lancet 2005; 365: 1552–1560. - PubMed
-
- Grandjean EM, Berthet P, Ruffmann R, et al. Efficacy of oral long-term N-acetylcysteine in chronic bronchopulmonary disease: a meta-analysis of published double-blind, placebo-controlled clinical trials. Clin Ther 2000; 22: 209–221. - PubMed
-
- Stey C, Steurer J, Bachmann S, et al. The effect of oral N-acetylcysteine in chronic bronchitis: a quantitative systematic review. Eur Respir J 2000; 16: 253–262. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical