

Should lung biopsies be performed in patients with severe asthma?
- PMID: 26324815
- PMCID: PMC9487699
- DOI: 10.1183/16000617.0045-2015
Should lung biopsies be performed in patients with severe asthma?
Abstract
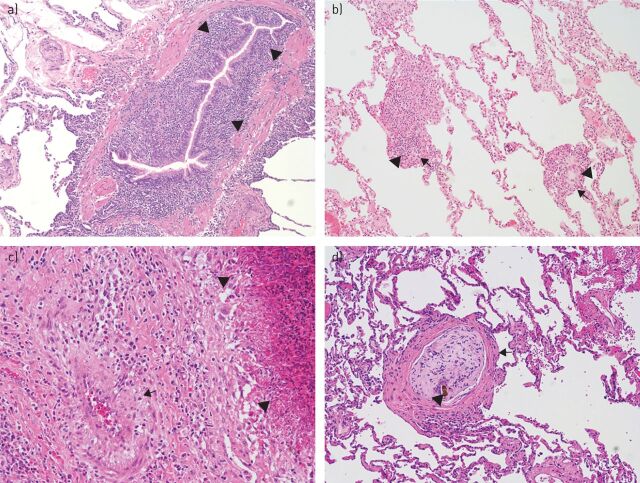
Asthma, and severe asthma, in particular, is increasingly recognised as a heterogeneous disease. Identifying these different phenotypes of asthma and assigning patients to phenotype-specific treatments is one of the current conundrums in respiratory medicine. Any diagnostic procedure in severe asthma (or any disease) should have two aims: 1) better understanding or identifying the diagnosis, and 2) providing information on the heterogeneity of asthma phenotypes to guide therapy with the objective of improving outcomes. Lung biopsies can target the large and small airways as well as the lung parenchyma. All compartments are affected in severe asthma; however, knowledge on the distal lung is limited. At this point, it remains uncertain whether lung specimens routinely add diagnostic information that is unable to be obtained otherwise. Indeed, whether a lung biopsy is indicated in the workup of a patient with severe asthma remains an individual decision. It is hoped this review will support rational decision-making and provide a detailed synopsis of the varied histopathological features seen in biopsies of patients with a diagnosis of severe asthma. Due to limited data on this topic this review is primarily based on opinion with recommendations arising primarily from the personal experience of the authors.
Copyright ©ERS 2015.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside the online version of this article at
Figures


Similar articles
-
New insights into the pathophysiology of the small airways in asthma.Clin Chest Med. 2006 Mar;27(1):41-52, vi. doi: 10.1016/j.ccm.2005.10.007. Clin Chest Med. 2006. PMID: 16543051 Review.
-
Asthma characteristics and biomarkers from the Airways Disease Endotyping for Personalized Therapeutics (ADEPT) longitudinal profiling study.Respir Res. 2015 Nov 17;16:142. doi: 10.1186/s12931-015-0299-y. Respir Res. 2015. PMID: 26576744 Free PMC article.
-
Asthma phenotypes today.Eur Ann Allergy Clin Immunol. 2013 Feb;45(1):17-24. Eur Ann Allergy Clin Immunol. 2013. PMID: 23678555 Review.
-
Characterizing asthma phenotypes: predictors and outcomes at the extremes of asthma severity.Respirology. 2009 Aug;14(6):778-80. doi: 10.1111/j.1440-1843.2009.01593.x. Respirology. 2009. PMID: 19703059 No abstract available.
-
Contribution of the distal lung to the pathologic and physiologic changes in asthma: potential therapeutic target Roger S. Mitchell lecture.Chest. 2003 Mar;123(3 Suppl):348S-55S. doi: 10.1378/chest.123.3_suppl.348s. Chest. 2003. PMID: 12628971 Review.
Cited by
-
Does transbronchial lung cryobiopsy give useful information in asthmatic patients?Multidiscip Respir Med. 2019 Apr 8;14:12. doi: 10.1186/s40248-019-0176-5. eCollection 2019. Multidiscip Respir Med. 2019. PMID: 30997044 Free PMC article.
-
Management of Severe Asthma before Referral to the Severe Asthma Specialist.J Allergy Clin Immunol Pract. 2017 Jul-Aug;5(4):877-886. doi: 10.1016/j.jaip.2017.04.027. J Allergy Clin Immunol Pract. 2017. PMID: 28689838 Free PMC article. Review.
-
Aberrant epithelial remodeling with impairment of cilia architecture in non-cystic fibrosis bronchiectasis.J Thorac Dis. 2018 Mar;10(3):1753-1764. doi: 10.21037/jtd.2018.02.13. J Thorac Dis. 2018. PMID: 29707330 Free PMC article.
-
The potential of omics approaches to elucidate mechanisms of biodiesel-induced pulmonary toxicity.Part Fibre Toxicol. 2019 Jan 8;16(1):4. doi: 10.1186/s12989-018-0284-y. Part Fibre Toxicol. 2019. PMID: 30621739 Free PMC article. Review.
-
Pulmonary inflammation promoted by type-2 dendritic cells is a feature of human and murine schistosomiasis.Nat Commun. 2023 Apr 3;14(1):1863. doi: 10.1038/s41467-023-37502-z. Nat Commun. 2023. PMID: 37012228 Free PMC article.
References
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention, revised 2014. Date last accessed: May 20, 2015. Date last updated: April 2015. www.ginasthma.org
-
- Wenzel SE. Asthma phenotypes: the evolution from clinical to molecular approaches. Nat Med 2012; 18: 716–725. - PubMed
-
- Wenzel SE. A plea to abandon asthma as a disease concept. Lancet 2006; 368: 705. - PubMed
-
- Cruschmann H. Ueber bronchiolitis exsudativa und ihr Verhaeltnis zum asthma nervosum. Dtsch Arch Klin Med 1882; 32: 1–34.
-
- Dolhnikoff M, da Silva LF, de Araujo BB, et al. . The outer wall of small airways is a major site of remodeling in fatal asthma. J Allergy Clin Immunol 2009; 123: 1090–1097. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical