

Do patients with a failed metal-on-metal hip implant with a pseudotumor present differences in their peripheral blood lymphocyte subpopulations?
- PMID: 26324830
- PMCID: PMC4626498
- DOI: 10.1007/s11999-015-4466-8
Do patients with a failed metal-on-metal hip implant with a pseudotumor present differences in their peripheral blood lymphocyte subpopulations?
Abstract
Background: Early adverse tissue reactions around metal-on-metal (MoM) hip replacements, especially pseudotumors, are a major concern. Because the causes and pathomechanisms of these pseudotumors remain largely unknown, clinical monitoring of patients with MoM bearings is challenging.
Questions/purposes: The purpose of this study was to compare the lymphocyte subpopulations in peripheral blood from patients with a failed MoM hip implant with and without a pseudotumor and patients with a well-functioning MoM hip implant without a pseudotumor. Potential differences in the systemic immune response are expected to reflect local differences in the periprosthetic tissues.
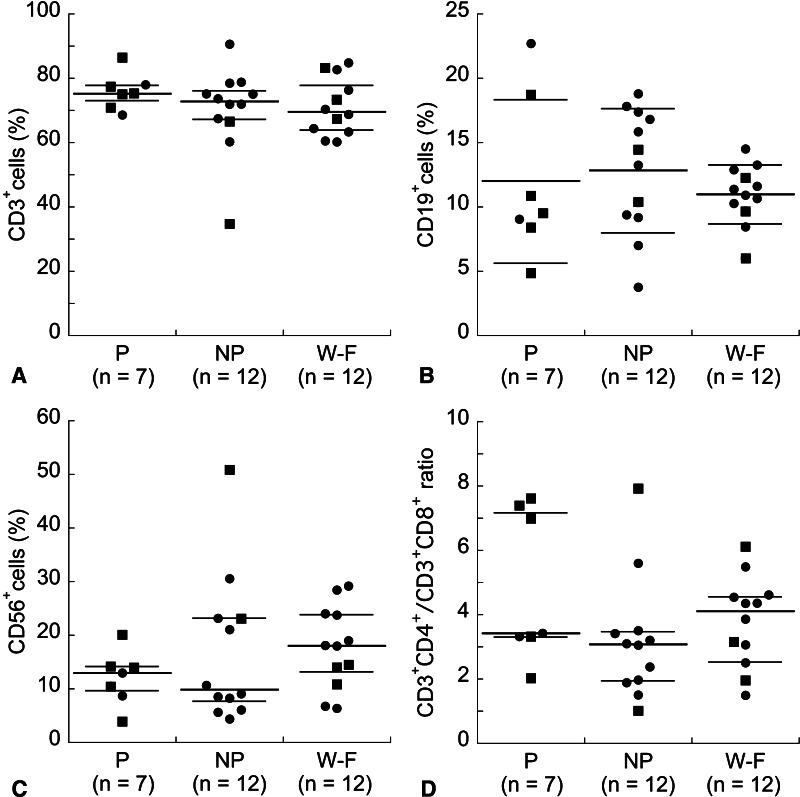
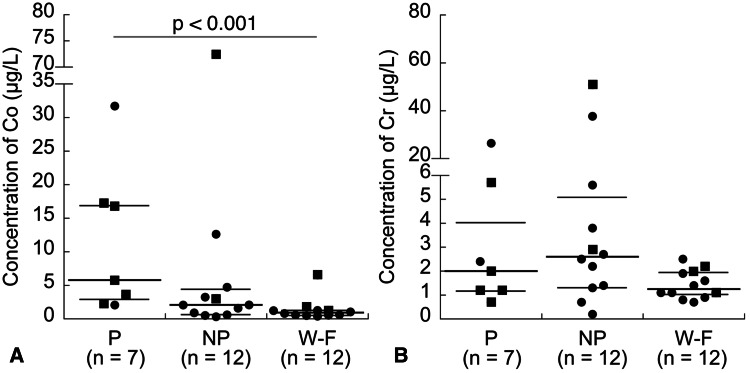
Methods: Consenting patients who underwent a revision of a failed MoM hip implant at The Ottawa Hospital (TOH) from 2011 to 2014, or presented with a well-functioning MoM hip implant for a postoperative clinical followup at TOH from 2012 to 2013, were recruited for this study, unless they met any of the exclusion criteria (including diagnosed conditions that can affect peripheral blood lymphocyte subpopulations). Patients with a failed implant were divided into two groups: those with a pseudotumor (two hip resurfacings and five total hip arthroplasties [THAs]) and those without a pseudotumor (10 hip resurfacings and two THAs). Patients with a well-functioning MoM hip implant (nine resurfacings and three THAs) at 5 or more years postimplantation and who did not have a pseudotumor as demonstrated sonographically served as the control group. Peripheral blood subpopulations of T cells (specifically T helper [Th] and cytotoxic T [Tc]), B cells, natural killer (NK) cells, memory T and B cells as well as type 1 (expressing interferon-γ) and type 2 (expressing interleukin-4) Th and Tc cells were analyzed by flow cytometry after immunostaining. Serum concentrations of cobalt and chromium were measured by inductively coupled plasma-mass spectrometry.
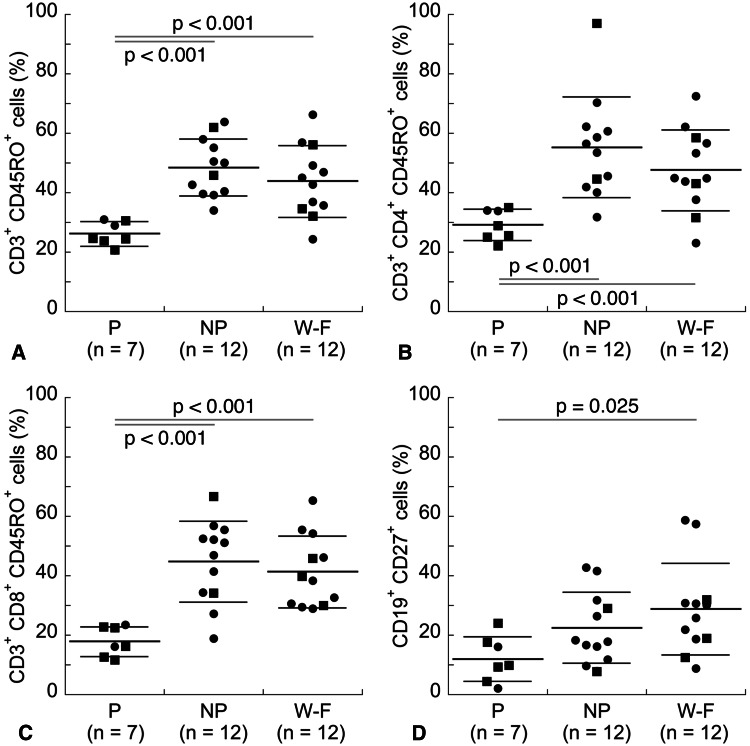
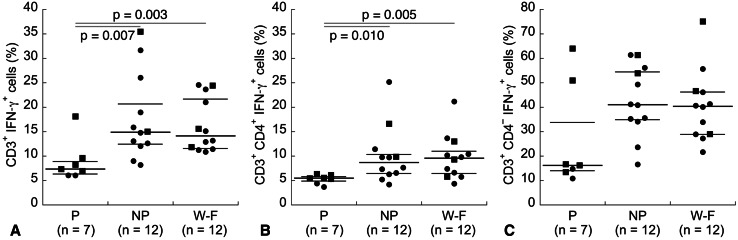
Results: The mean percentages of total memory T cells and, specifically, memory Th and memory Tc cells were lower in patients with a failed MoM hip implant with a pseudotumor than in both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (memory Th cells: 29% ± 5% [means ± SD] versus 55% ± 17%, d = 1.8, 95% confidence interval [CI] [1.2, 2.5] and versus 48% ± 14%, d = 1.6, 95% CI [1.0, 2.2], respectively; memory Tc cells: 18% ± 5% versus 45% ± 14%, d = 2.3, 95% CI [1.5, 3.1] and versus 41% ± 12%, d = 2.3, 95% CI [1.5, 3.1], respectively; p < 0.001 in all cases). The mean percentage of memory B cells was also lower in patients with a failed MoM hip implant with a pseudotumor than in patients with a well-functioning implant without a pseudotumor (12% ± 8% versus 29% ± 16%, d = 1.3, 95% CI [0.7, 1.8], p = 0.025). In addition, patients with a failed MoM hip implant with a pseudotumor had overall lower percentages of type 1 Th cells than both patients with a failed implant without a pseudotumor and patients with a well-functioning implant without a pseudotumor (5.5% [4.9%-5.8%] [median with interquartile range] versus 8.7% [6.5%-10.2%], d = 1.4, 95% CI [0.8, 2.0] and versus 9.6% [6.4%-11.1%], d = 1.6, 95% CI [1.0, 2.2], respectively; p ≤ 0.010 in both cases). Finally, serum cobalt concentrations in patients with a failed MoM hip implant with a pseudotumor were overall higher than those in patients with a well-functioning implant without a pseudotumor (5.8 µg/L [2.9-17.0 µg/L] versus 0.9 µg/L [0.6-1.3 µg/L], d = 2.2, 95% CI [1.4, 2.9], p < 0.001).
Conclusions: Overall, results suggest the presence of a type IV hypersensitivity reaction, with a predominance of type 1 Th cells, in patients with a failed MoM hip implant with a pseudotumor.
Clinical relevance: The lower percentages of memory T cells (specifically Th and Tc) as well as type 1 Th cells in peripheral blood of patients with a failed MoM hip implant with a pseudotumor could potentially become diagnostic biomarkers for the detection of pseudotumors. Although implant design (hip resurfacing or THA) did not seem to affect the results, as suggested by the scatter of the data with respect to this parameter, future studies with additional patients could include the analysis of implant design in addition to correlations with histological analyses of specific Th subsets in periprosthetic tissues.
Figures
Comment in
-
CORR Insights(®): do patients with a failed metal-on-metal hip implant with a pseudotumor present differences in their peripheral blood lymphocyte subpopulations?Clin Orthop Relat Res. 2015 Dec;473(12):3915-7. doi: 10.1007/s11999-015-4571-8. Clin Orthop Relat Res. 2015. PMID: 26463565 Free PMC article. No abstract available.
References
-
- Bisschop R, Boomsma MF, Van Raay JJ, Tiebosch AT, Maas M, Gerritsma CL. High prevalence of pseudotumors in patients with a Birmingham Hip Resurfacing prosthesis: a prospective cohort study of one hundred and twenty-nine patients. J Bone Joint Surg Am. 2013;95:1554–1560. doi: 10.2106/JBJS.L.00716. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
