

High Risk of Failure With Bimodular Femoral Components in THA
- PMID: 26324837
- PMCID: PMC4686519
- DOI: 10.1007/s11999-015-4542-0
High Risk of Failure With Bimodular Femoral Components in THA
Abstract
Background: The bimodular femoral neck implant (modularity in the neck section and prosthetic head) offers several implant advantages to the surgeon performing THAs, however, there have been reports of failure of bimodular femoral implants involving neck fractures or adverse tissue reaction to metal debris. We aimed to assess the results of the bimodular implants used in the THAs we performed.
Questions/purposes: We asked: (1) What is the survivorship of the PROFEMUR(®) bimodular femoral neck stems? (2) What are the modes of failure of this bimodular femoral neck implant? (3) What are the major risk factors for the major modes of failure of this device?
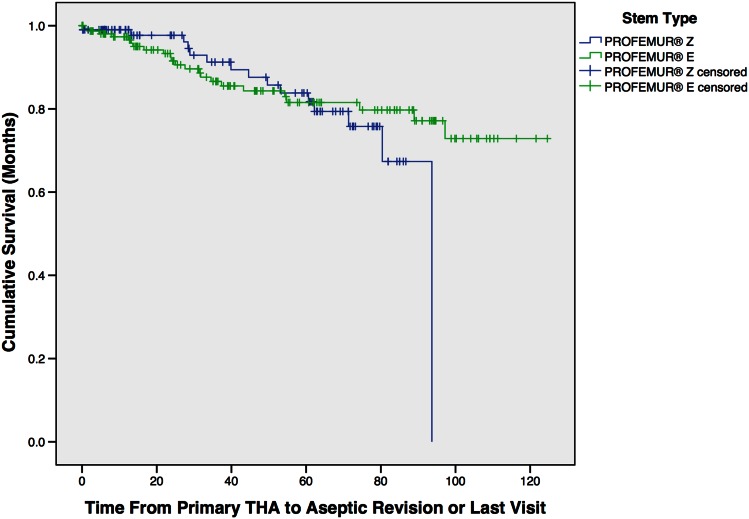
Methods: Between 2003 and 2009, we used one family of bimodular femoral neck stems for all primary THAs (PROFEMUR(®) Z and PROFEMUR(®) E). During this period, 277 THAs (in 242 patients) were performed with these implants. One hundred seventy were done with the bimodular PROFEMUR(®) E (all are accounted for here), and when that implant was suspected of having a high risk of failure, the bimodular PROFEMUR(®) Z was used instead. One hundred seven THAs were performed using this implant (all are accounted for in this study). All bearing combinations, including metal-on-metal, metal-on-polyethylene, and ceramic-on-ceramic, are included here. Data for the cohort included patient demographics, BMI, implant dimensions, type of articular surface, length of followup, and C-reactive protein serum level. We assessed survivorship of the two stems using Kaplan-Meier curves and determined the frequency of the different modes of stem failure. For each of the major modes of failure, we performed binary logistic regression to identify associated risk factors.
Results: Survivorship of the stems, using aseptic revision as the endpoint, was 85% for the patients with the PROFEMUR(®) E stems with a mean followup of 50 months (range, 1-125 months) and 85% for the PROFEMUR(®) Z with a mean followup of 50 months (range, 1-125 months)(95% CI, 74-87 months). The most common modes of failure were loosening (9% for the PROFEMUR(®) E), neck fracture (6% for the PROFEMUR(®) Z and 0.6% for the PROFEMUR(®) E), metallosis (1%), and periprosthetic fracture (1%). Only the bimodular PROFEMUR(®) E was associated with femoral stem loosening (odds ratio [OR] =1.1; 95% CI, 1.04-1.140; p = 0.032). Larger head (OR = 3.2; 95% CI, 0.7-14; p = 0.096), BMI (OR = 1.19; 95% CI, 1-1.4; p = 0.038) and total offset (OR = 1.83; 95% CI, 1.13-2.9; p = 0.039) were associated with neck fracture.
Conclusion: Bimodular neck junctions may be potentiated by long neck lengths, greater offset, and larger head diameters. These factors may contribute to bimodular neck failure by creating a larger moment about the neck's insertion in the stem. The PROFEMUR(®) E implant is associated with high periprosthetic loosening. Based on our experience we cannot recommend the use of bimodular femoral neck implants.
Level of evidence: Level III, therapeutic study.
Figures

Comment in
-
CORR Insights(®): High Risk of Failure With Bimodular Femoral Components in THA.Clin Orthop Relat Res. 2016 Jan;474(1):154-5. doi: 10.1007/s11999-015-4568-3. Epub 2015 Sep 25. Clin Orthop Relat Res. 2016. PMID: 26407701 Free PMC article. No abstract available.
References
-
- Australian Orthopaedic Association National Joint Replacement Registry. Annual Report 2012. Available at: https://aoanjrr.dmac.adelaide.edu.au/en/annual-reports-2012. Accessed June 11, 2015.
-
- Australian Orthopaedic Association National Joint Replacement Registry. Annual Report 2013. Available at: https://aoanjrr.dmac.adelaide.edu.au/en/annual-reports-2013. Accessed June 11, 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
