

International study of the place of death of people with cancer: a population-level comparison of 14 countries across 4 continents using death certificate data
- PMID: 26325102
- PMCID: PMC4815784
- DOI: 10.1038/bjc.2015.312
International study of the place of death of people with cancer: a population-level comparison of 14 countries across 4 continents using death certificate data
Abstract
Background: Where people die can influence a number of indicators of the quality of dying. We aimed to describe the place of death of people with cancer and its associations with clinical, socio-demographic and healthcare supply characteristics in 14 countries.
Methods: Cross-sectional study using death certificate data for all deaths from cancer (ICD-10 codes C00-C97) in 2008 in Belgium, Canada, Czech Republic, England, France, Hungary, Italy, Mexico, the Netherlands, New Zealand, South Korea, Spain (2010), USA (2007) and Wales (N=1,355,910). Multivariable logistic regression analyses evaluated factors associated with home death within countries and differences across countries.
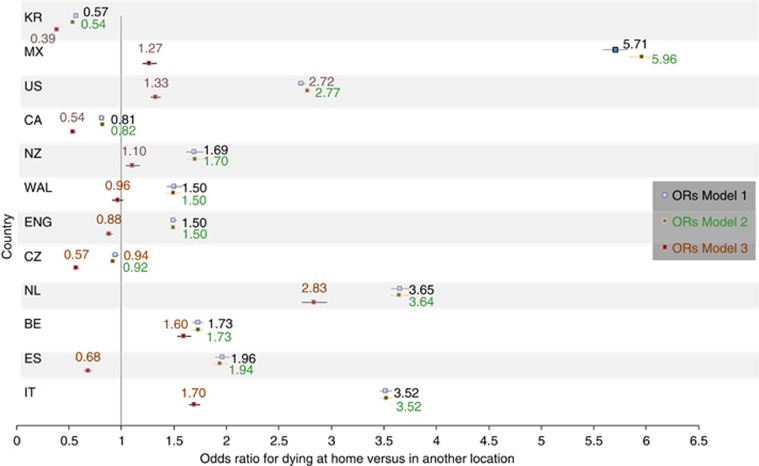
Results: Between 12% (South Korea) and 57% (Mexico) of cancer deaths occurred at home; between 26% (Netherlands, New Zealand) and 87% (South Korea) occurred in hospital. The large between-country differences in home or hospital deaths were partly explained by differences in availability of hospital- and long-term care beds and general practitioners. Haematologic rather than solid cancer (odds ratios (ORs) 1.29-3.17) and being married rather than divorced (ORs 1.17-2.54) were most consistently associated with home death across countries.
Conclusions: A large country variation in the place of death can partly be explained by countries' healthcare resources. Country-specific choices regarding the organisation of end-of-life cancer care likely explain an additional part. These findings indicate the further challenge to evaluate how different specific policies can influence place of death patterns.
Figures
References
-
- Boockvar K, Fishman E, Kyriacou CK, Monias A, Gavi S, Cortes T (2014) Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med 164: 545–550. - PubMed
-
- Brown M, Colton T (2001) Dying epistemologies: an analysis of home death and its critique. Environ Plan 33: 799–821.
-
- Centeno C, Pons JJ, Lynch T, Donea O, Rocafort J, Clark D (2013) EAPC atlas of palliative care in Europe - Cartographic edition. EAPC Press: Milan.
-
- Cleary J, De Lima L, Eisenchlas J, Radbruch L, Torode J, Cherny NI (2013. a) Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in Latin America and the Caribbean: a report from the Global Opioid Policy Initiative (GOPI). Ann Oncol 24(Suppl 1): 41–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
