

Ability to Generate Patient-Derived Breast Cancer Xenografts Is Enhanced in Chemoresistant Disease and Predicts Poor Patient Outcomes
- PMID: 26325287
- PMCID: PMC4556673
- DOI: 10.1371/journal.pone.0136851
Ability to Generate Patient-Derived Breast Cancer Xenografts Is Enhanced in Chemoresistant Disease and Predicts Poor Patient Outcomes
Erratum in
-
Correction: Ability to Generate Patient-Derived Breast Cancer Xenografts Is Enhanced in Chemoresistant Disease and Predicts Poor Patient Outcomes.PLoS One. 2016 Mar 8;11(3):e0151121. doi: 10.1371/journal.pone.0151121. eCollection 2016. PLoS One. 2016. PMID: 26953790 Free PMC article. No abstract available.
Abstract
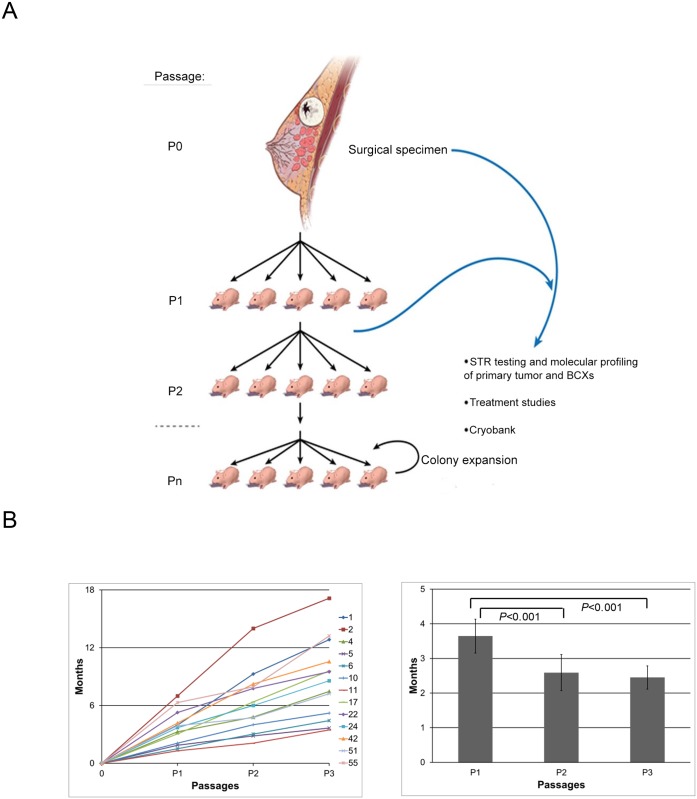
Background: Breast cancer patients who are resistant to neoadjuvant chemotherapy (NeoCT) have a poor prognosis. There is a pressing need to develop in vivo models of chemo resistant tumors to test novel therapeutics. We hypothesized that patient-derived breast cancer xenografts (BCXs) from chemo- naïve and chemotherapy-exposed tumors can provide high fidelity in vivo models for chemoresistant breast cancers.
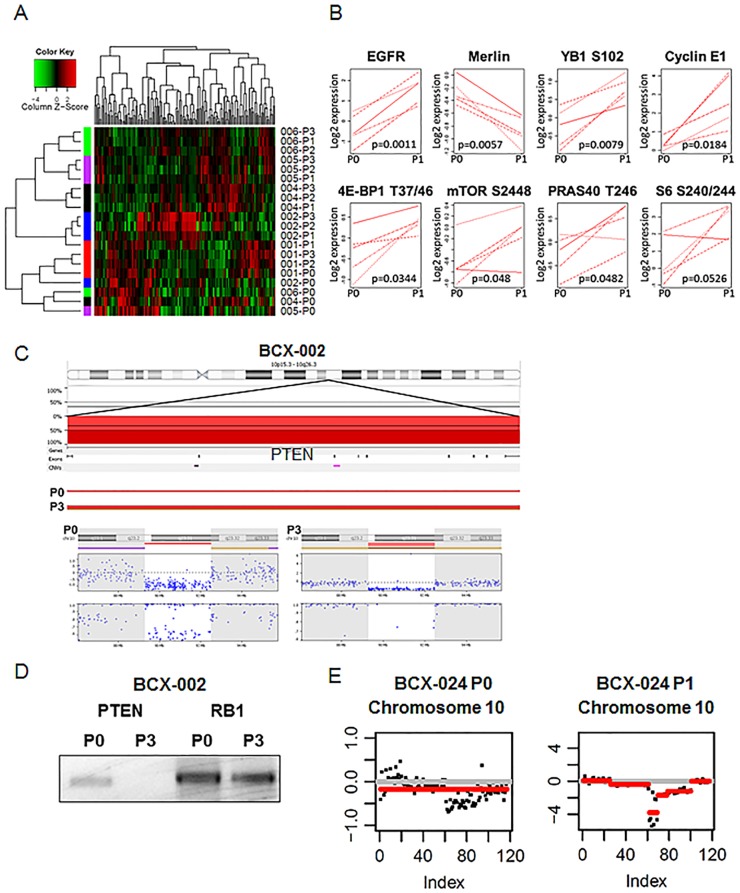
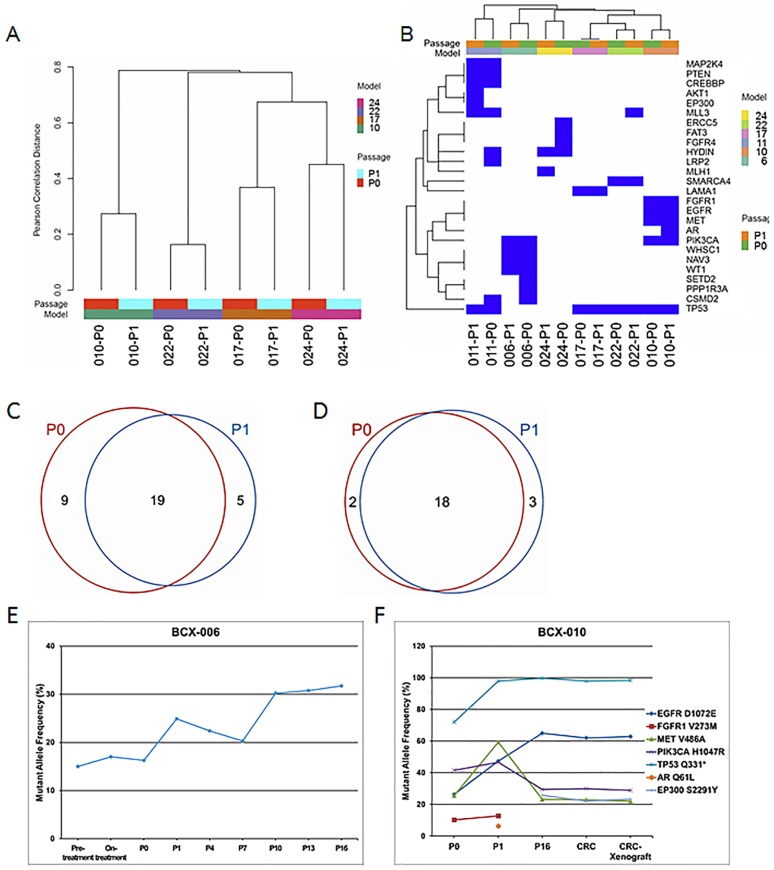
Methods: Patient tumors and BCXs were characterized with short tandem repeat DNA fingerprinting, reverse phase protein arrays, molecular inversion probe arrays, and next generation sequencing.
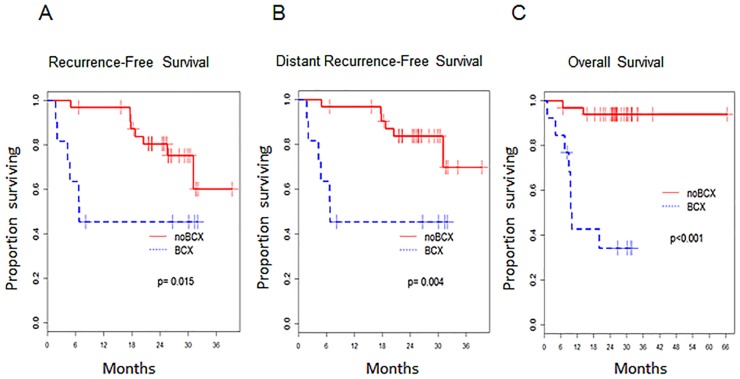
Results: Forty-eight breast cancers (24 post-chemotherapy, 24 chemo-naïve) were implanted and 13 BCXs were established (27%). BCX engraftment was higher in TNBC compared to hormone-receptor positive cancer (53.8% vs. 15.6%, p = 0.02), in tumors from patients who received NeoCT (41.7% vs. 8.3%, p = 0.02), and in patients who had progressive disease on NeoCT (85.7% vs. 29.4%, p = 0.02). Twelve patients developed metastases after surgery; in five, BCXs developed before distant relapse. Patients whose tumors developed BCXs had a lower recurrence-free survival (p = 0.015) and overall survival (p<0.001). Genomic losses and gains could be detected in the BCX, and three models demonstrated a transformation to induce mouse tumors. However, overall, somatic mutation profiles including potential drivers were maintained upon implantation and serial passaging. One BCX model was cultured in vitro and re-implanted, maintaining its genomic profile.
Conclusions: BCXs can be established from clinically aggressive breast cancers, especially in TNBC patients with poor response to NeoCT. Future studies will determine the potential of in vivo models for identification of genotype-phenotype correlations and individualization of treatment.
Conflict of interest statement
Figures
References
-
- Kuerer HM, Newman LA, Smith TL, Ames FC, Hunt KK, Dhingra K, et al. Clinical course of breast cancer patients with complete pathologic primary tumor and axillary lymph node response to doxorubicin-based neoadjuvant chemotherapy. J Clin Oncol. 1999;17(2):460–9. Epub 1999/03/18. . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
