

CD34-Selected Allogeneic Hematopoietic Stem Cell Transplantation for Patients with Relapsed, High-Risk Multiple Myeloma
- PMID: 26325439
- PMCID: PMC4975432
- DOI: 10.1016/j.bbmt.2015.08.025
CD34-Selected Allogeneic Hematopoietic Stem Cell Transplantation for Patients with Relapsed, High-Risk Multiple Myeloma
Abstract
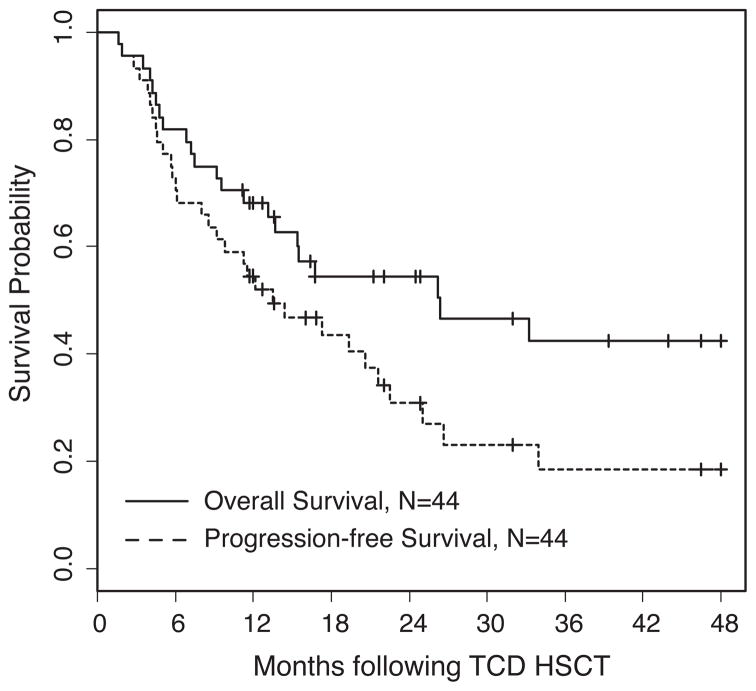
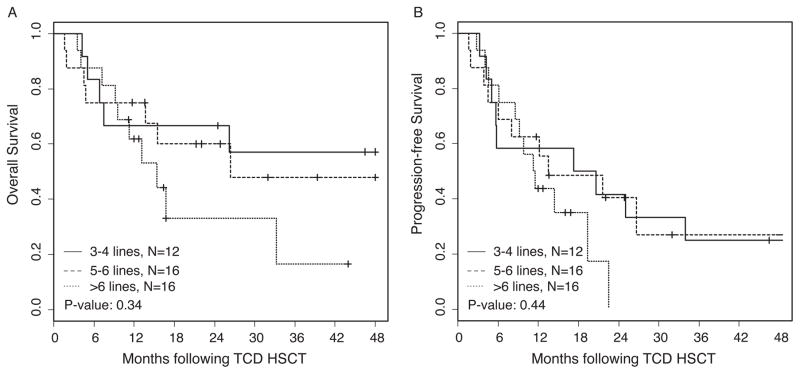
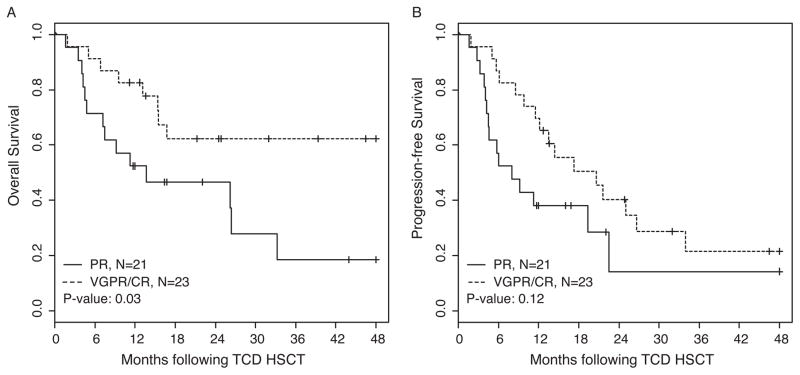
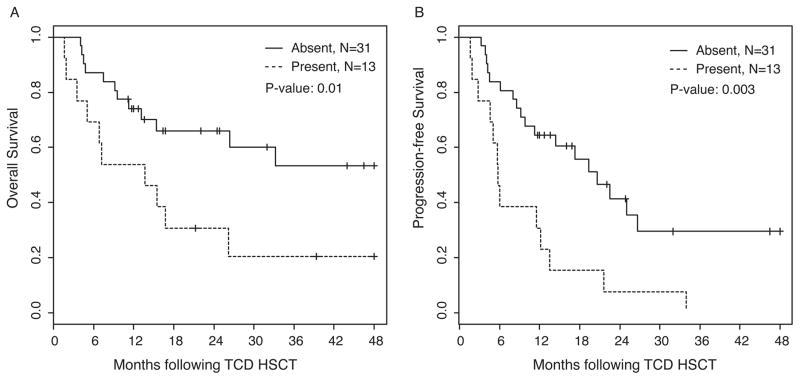
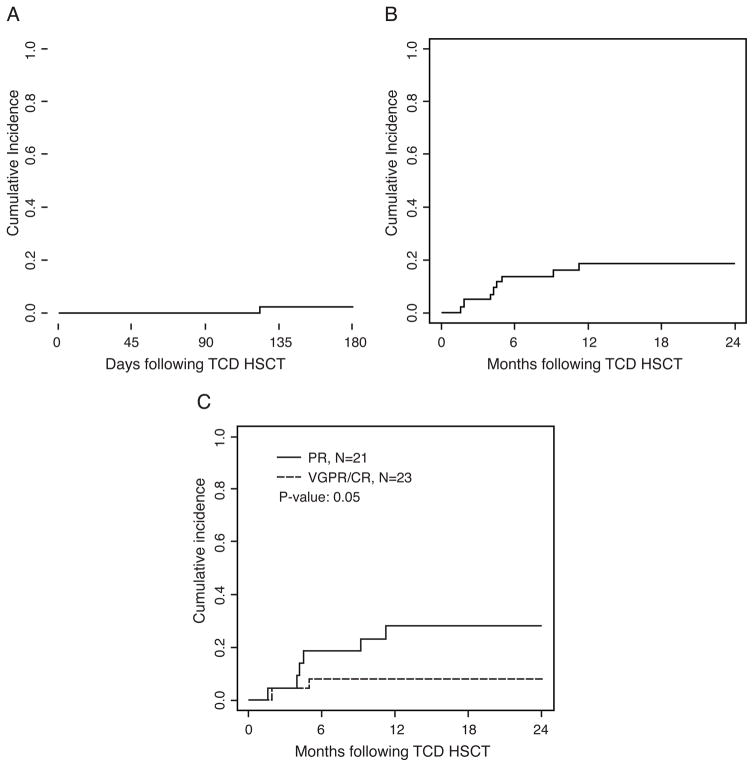
We report results of a retrospective analysis of 44 patients with relapsed and high-risk multiple myeloma (MM) undergoing allogeneic CD34-selected hematopoietic stem cell transplantation (HSCT) from HLA-compatible donors. Patients had multiply relapsed disease including relapse at <15 months after autologous transplantation and most patients (28 of 44; 65%) also had high-risk cytogenetics. Before transplantation, patients received busulfan (.8 mg/kg × 10 doses), melphalan (70 mg/m(2) × 2 days), fludarabine (25 mg/m(2) × 5 days), and rabbit antithymocyte globulin (2.5 mg/kg × 2 days). Patients with 10/10 HLA- matched donors were treated prophylactically with low doses of donor lymphocyte infusions (.5 to 1 × 10(6) CD3(+)/kg) starting 4 to 6 months after CD34-selected HSCT. Acute (grade II to IV) graft-versus-host disease (GVHD) and transplantation-related mortality at 12 months were 2% and 18%, respectively. Chronic GVHD was not observed in any patient. Overall and progression-free survival at 2 years were 54% and 31%, respectively. By multivariate analyses, the outcomes of CD34-selected HSCT were influenced by presence of extramedullary disease, disease status before CD34-selected HSCT, and age. This study demonstrates notable safety and efficacy of CD34-selected HSCT in patients with multiply relapsed MM, including those with high-risk cytogenetics.
Keywords: Adoptive immunotherapy; D34-selected hematopoietic stem cell transplantation; Relapsed high-risk multiple myeloma.
Copyright © 2016 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Kyle RA, Rajkumar SV. Multiple myeloma. N Engl J Med. 2004;351(18):1860–1873. - PubMed
-
- Smith BD, Smith GL, Hurria A, Hortobagyi GN, Buchholz TA. Future of cancer incidence in the United States: burdens upon an aging, changing nation. J Clin Oncol. 2009;27(17):2758–2765. - PubMed
-
- Rajkumar S, Fonseca R, Lacy M, et al. Abnormal cytogenetics predict poor survival after high-dose therapy and autologous blood cell transplantation in multiple myeloma. Bone Marrow Transplant. 1999;24(5):497–503. - PubMed
-
- Gahrton G, Tura S, Ljungman P, et al. Allogeneic bone marrow transplantation in multiple myeloma. European Group for Bone Marrow Transplantation. N Engl J Med. 1991;325(18):1267–1273. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
