

Integrative Clinical Sequencing in the Management of Refractory or Relapsed Cancer in Youth
- PMID: 26325560
- PMCID: PMC4758114
- DOI: 10.1001/jama.2015.10080
Integrative Clinical Sequencing in the Management of Refractory or Relapsed Cancer in Youth
Abstract
Importance: Cancer is caused by a diverse array of somatic and germline genomic aberrations. Advances in genomic sequencing technologies have improved the ability to detect these molecular aberrations with greater sensitivity. However, integrating them into clinical management in an individualized manner has proven challenging.
Objective: To evaluate the use of integrative clinical sequencing and genetic counseling in the assessment and treatment of children and young adults with cancer.
Design, setting, and participants: Single-site, observational, consecutive case series (May 2012-October 2014) involving 102 children and young adults (mean age, 10.6 years; median age, 11.5 years, range, 0-22 years) with relapsed, refractory, or rare cancer.
Exposures: Participants underwent integrative clinical exome (tumor and germline DNA) and transcriptome (tumor RNA) sequencing and genetic counseling. Results were discussed by a precision medicine tumor board, which made recommendations to families and their physicians.
Main outcomes and measures: Proportion of patients with potentially actionable findings, results of clinical actions based on integrative clinical sequencing, and estimated proportion of patients or their families at risk of future cancer.
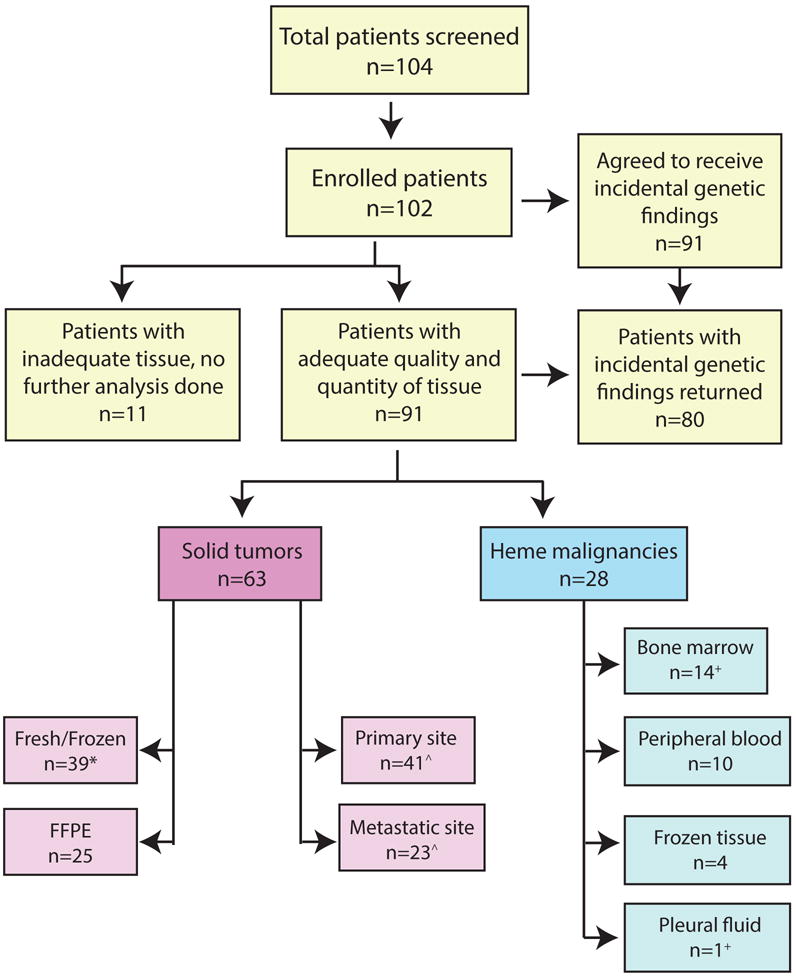
Results: Of the 104 screened patients, 102 enrolled with 91 (89%) having adequate tumor tissue to complete sequencing. Only the 91 patients were included in all calculations, including 28 (31%) with hematological malignancies and 63 (69%) with solid tumors. Forty-two patients (46%) had actionable findings that changed their cancer management: 15 of 28 (54%) with hematological malignancies and 27 of 63 (43%) with solid tumors. Individualized actions were taken in 23 of the 91 (25%) based on actionable integrative clinical sequencing findings, including change in treatment for 14 patients (15%) and genetic counseling for future risk for 9 patients (10%). Nine of 91 (10%) of the personalized clinical interventions resulted in ongoing partial clinical remission of 8 to 16 months or helped sustain complete clinical remission of 6 to 21 months. All 9 patients and families with actionable incidental genetic findings agreed to genetic counseling and screening.
Conclusions and relevance: In this single-center case series involving young patients with relapsed or refractory cancer, incorporation of integrative clinical sequencing data into clinical management was feasible, revealed potentially actionable findings in 46% of patients, and was associated with change in treatment and family genetic counseling for a small proportion of patients. The lack of a control group limited assessing whether better clinical outcomes resulted from this approach than outcomes that would have occurred with standard care.
Conflict of interest statement
Figures

Comment in
-
Improving Patient Outcomes With Cancer Genomics: Unique Opportunities and Challenges in Pediatric Oncology.JAMA. 2015 Sep 1;314(9):881-3. doi: 10.1001/jama.2015.9794. JAMA. 2015. PMID: 26325556 Free PMC article. No abstract available.
-
Translational Childhood Cancer Genomics: The Future Is Now.JAMA Oncol. 2016 Mar;2(3):384-5. doi: 10.1001/jamaoncol.2015.5076. JAMA Oncol. 2016. PMID: 26747469 No abstract available.
Similar articles
-
Discovery of actionable genetic alterations with targeted panel sequencing in children with relapsed or refractory solid tumors.PLoS One. 2019 Nov 20;14(11):e0224227. doi: 10.1371/journal.pone.0224227. eCollection 2019. PLoS One. 2019. PMID: 31747416 Free PMC article.
-
MultiDimensional ClinOmics for Precision Therapy of Children and Adolescent Young Adults with Relapsed and Refractory Cancer: A Report from the Center for Cancer Research.Clin Cancer Res. 2016 Aug 1;22(15):3810-20. doi: 10.1158/1078-0432.CCR-15-2717. Epub 2016 Mar 18. Clin Cancer Res. 2016. PMID: 26994145 Free PMC article.
-
Molecular Profiling of Hard-to-Treat Childhood and Adolescent Cancers.JAMA Netw Open. 2019 Apr 5;2(4):e192906. doi: 10.1001/jamanetworkopen.2019.2906. JAMA Netw Open. 2019. PMID: 31026031 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
A 2015 update on predictive molecular pathology and its role in targeted cancer therapy: a review focussing on clinical relevance.Cancer Gene Ther. 2015 Sep;22(9):417-30. doi: 10.1038/cgt.2015.39. Epub 2015 Sep 11. Cancer Gene Ther. 2015. PMID: 26358176 Review.
Cited by
-
Clinical Sequencing Exploratory Research Consortium: Accelerating Evidence-Based Practice of Genomic Medicine.Am J Hum Genet. 2016 Jun 2;98(6):1051-1066. doi: 10.1016/j.ajhg.2016.04.011. Epub 2016 May 12. Am J Hum Genet. 2016. PMID: 27181682 Free PMC article.
-
Recent advances in genetic predisposition to pediatric acute lymphoblastic leukemia.Expert Rev Hematol. 2020 Jan;13(1):55-70. doi: 10.1080/17474086.2020.1685866. Epub 2019 Nov 19. Expert Rev Hematol. 2020. PMID: 31657974 Free PMC article. Review.
-
Cascading After Peridiagnostic Cancer Genetic Testing: An Alternative to Population-Based Screening.J Clin Oncol. 2020 May 1;38(13):1398-1408. doi: 10.1200/JCO.19.02010. Epub 2020 Jan 10. J Clin Oncol. 2020. PMID: 31922925 Free PMC article.
-
Pursuing Precision: Receptor Tyrosine Kinase Inhibitors for Treatment of Pediatric Solid Tumors.Cancers (Basel). 2021 Jul 14;13(14):3531. doi: 10.3390/cancers13143531. Cancers (Basel). 2021. PMID: 34298746 Free PMC article. Review.
-
Mutation Detection in Patients With Advanced Cancer by Universal Sequencing of Cancer-Related Genes in Tumor and Normal DNA vs Guideline-Based Germline Testing.JAMA. 2017 Sep 5;318(9):825-835. doi: 10.1001/jama.2017.11137. JAMA. 2017. PMID: 28873162 Free PMC article.
References
-
- Moroz V, Machin D, Faldum A, et al. Changes over three decades in outcome and the prognostic influence of age-at-diagnosis in young patients with neuroblastoma: a report from the International Neuroblastoma Risk Group Project. European journal of cancer. 2011 Mar;47(4):561–571. - PubMed
-
- Oberlin O, Rey A, Lyden E, et al. Prognostic factors in metastatic rhabdomyosarcomas: results of a pooled analysis from United States and European cooperative groups. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2008 May 10;26(14):2384–2389. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
