

Pulmonary ultrasound and pulse oximetry versus chest radiography and arterial blood gas analysis for the diagnosis of acute respiratory distress syndrome: a pilot study
- PMID: 26325623
- PMCID: PMC4511255
- DOI: 10.1186/s13054-015-0995-5
Pulmonary ultrasound and pulse oximetry versus chest radiography and arterial blood gas analysis for the diagnosis of acute respiratory distress syndrome: a pilot study
Abstract
Introduction: In low-resource settings it is not always possible to acquire the information required to diagnose acute respiratory distress syndrome (ARDS). Ultrasound and pulse oximetry, however, may be available in these settings. This study was designed to test whether pulmonary ultrasound and pulse oximetry could be used in place of traditional radiographic and oxygenation evaluation for ARDS.
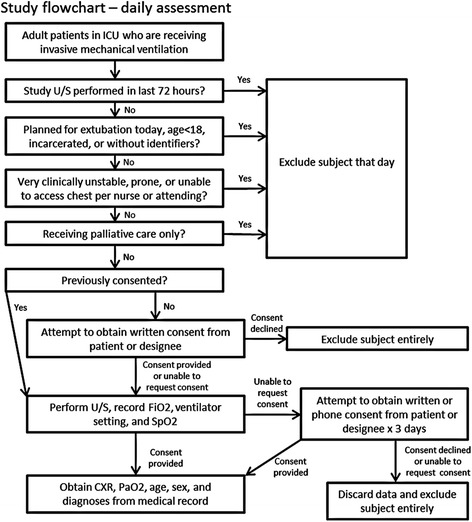
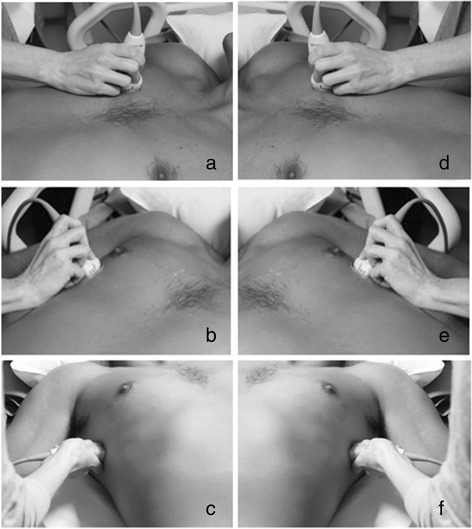
Methods: This study was a prospective, single-center study in the ICU of Harborview Medical Center, a referral hospital in Seattle, Washington, USA. Bedside pulmonary ultrasound was performed on ICU patients receiving invasive mechanical ventilation. Pulse oximetric oxygen saturation (SpO2), partial pressure of oxygen (PaO2), fraction of inspired oxygen (FiO2), provider diagnoses, and chest radiograph closest to time of ultrasound were recorded or interpreted.
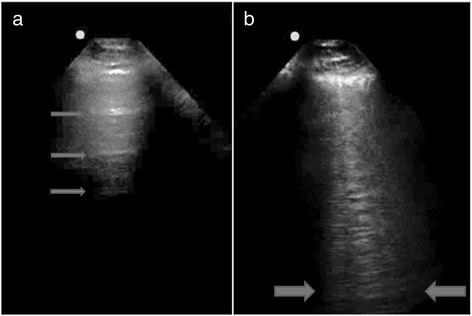
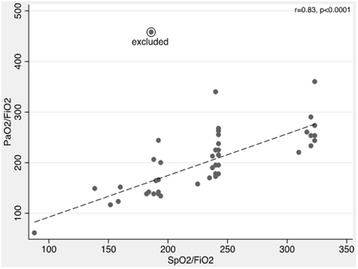
Results: One hundred and twenty three ultrasound assessments were performed on 77 consecutively enrolled patients with respiratory failure. Oxygenation and radiographic criteria for ARDS were met in 35 assessments. Where SpO2 ≤ 97%, the Spearman rank correlation coefficient between SpO2/FiO2 and PaO2/FiO2 was 0.83, p < 0.0001. The sensitivity and specificity of the previously reported threshold of SpO2/FiO2 ≤ 315 for PaO2/FiO2 ≤ 300 was 83% (95% confidence interval (CI) 68-93), and 50% (95% CI 1-99), respectively. Sensitivity and specificity of SpO2/FiO2 ≤ 235 for PaO2/FiO2 ≤ 200 was 70% (95% CI 47-87), and 90% (95% CI 68-99), respectively. For pulmonary ultrasound assessments interpreted by the study physician, the sensitivity and specificity of ultrasound interstitial syndrome bilaterally and involving at least three lung fields were 80% (95% CI 63-92) and 62% (95% CI 49-74) for radiographic criteria for ARDS. Combining SpO2/FiO2 with ultrasound to determine oxygenation and radiographic criteria for ARDS, the sensitivity was 83% (95% CI 52-98) and specificity was 62% (95% CI 38-82). For moderate-severe ARDS criteria (PaO2/FiO2 ≤ 200), sensitivity was 64% (95% CI 31-89) and specificity was 86% (95% CI 65-97). Excluding repeat assessments and independent interpretation of ultrasound images did not significantly alter the sensitivity measures.
Conclusions: Pulse oximetry and pulmonary ultrasound may be useful tools to screen for, or rule out, impaired oxygenation or lung abnormalities consistent with ARDS in under-resourced settings where arterial blood gas testing and chest radiography are not readily available.
Figures
References
-
- Riviello E, Talmor D, Novack V, Kiviri W, Twagirumugabe T, Banner-Goodspeed V, et al. Incidence and outcomes of ARDS in Rwanda using modified Berlin criteria for resource-poor settings. Crit Care Med. 2014;42:A1447–8. doi: 10.1097/01.ccm.0000457860.12587.ff. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
