

Rapid Diagnosis of Infection in the Critically Ill, a Multicenter Study of Molecular Detection in Bloodstream Infections, Pneumonia, and Sterile Site Infections
- PMID: 26327198
- PMCID: PMC4603364
- DOI: 10.1097/CCM.0000000000001249
Rapid Diagnosis of Infection in the Critically Ill, a Multicenter Study of Molecular Detection in Bloodstream Infections, Pneumonia, and Sterile Site Infections
Abstract
Objective: Early identification of causative microorganism(s) in patients with severe infection is crucial to optimize antimicrobial use and patient survival. However, current culture-based pathogen identification is slow and unreliable such that broad-spectrum antibiotics are often used to insure coverage of all potential organisms, carrying risks of overtreatment, toxicity, and selection of multidrug-resistant bacteria. We compared the results obtained using a novel, culture-independent polymerase chain reaction/electrospray ionization-mass spectrometry technology with those obtained by standard microbiological testing and evaluated the potential clinical implications of this technique.
Design: Observational study.
Setting: Nine ICUs in six European countries.
Patients: Patients admitted between October 2013 and June 2014 with suspected or proven bloodstream infection, pneumonia, or sterile fluid and tissue infection were considered for inclusion.
Interventions: None.
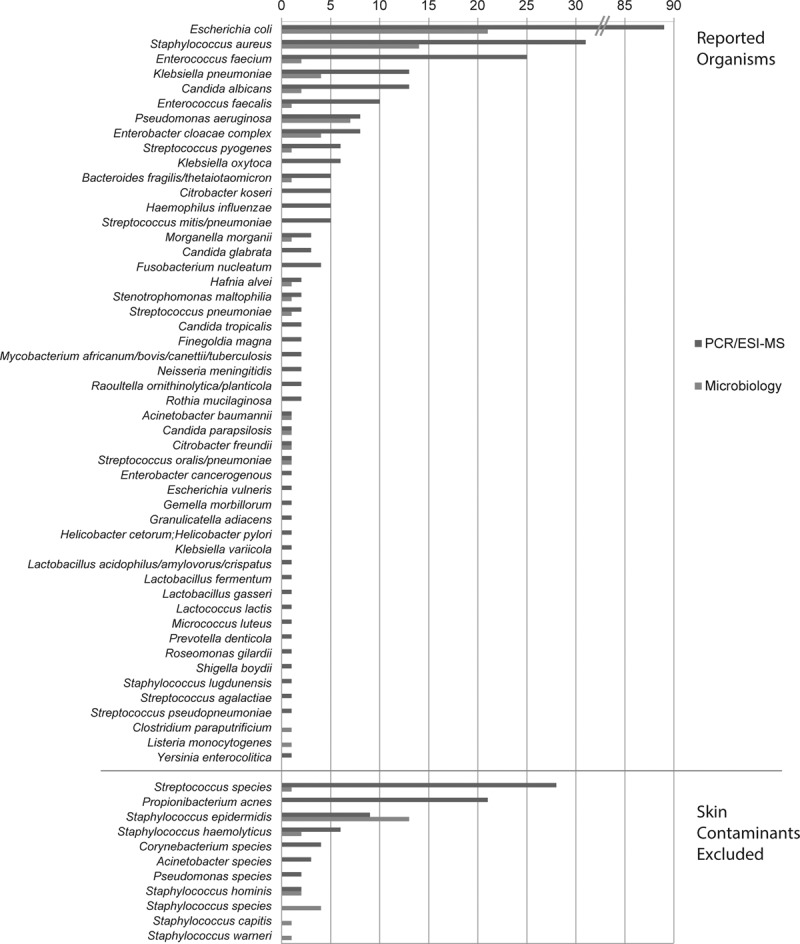
Measurements and main results: We tested 616 bloodstream infection, 185 pneumonia, and 110 sterile fluid and tissue specimens from 529 patients. From the 616 bloodstream infection samples, polymerase chain reaction/electrospray ionization-mass spectrometry identified a pathogen in 228 cases (37%) and culture in just 68 (11%). Culture was positive and polymerase chain reaction/electrospray ionization-mass spectrometry negative in 13 cases, and both were negative in 384 cases, giving polymerase chain reaction/electrospray ionization-mass spectrometry a sensitivity of 81%, specificity of 69%, and negative predictive value of 97% at 6 hours from sample acquisition. The distribution of organisms was similar with both techniques. Similar observations were made for pneumonia and sterile fluid and tissue specimens. Independent clinical analysis of results suggested that polymerase chain reaction/electrospray ionization-mass spectrometry technology could potentially have resulted in altered treatment in up to 57% of patients.
Conclusions: Polymerase chain reaction/electrospray ionization-mass spectrometry provides rapid pathogen identification in critically ill patients. The ability to rule out infection within 6 hours has potential clinical and economic benefits.
Conflict of interest statement
Dr. Vincent’s institution received financial support from Abbott. Dr. Brealey received financial support from Abbott to conduct and present this study at international meetings (travel expenses and lecture fees) and disclosed off-label product use (now Conformité Européene [CE] marked for use in Europe alone). His institution received financial support. Dr. Libert’s institution received financial support from Abbott (received support for travel to meetings for the study). Dr. Abidi disclosed work for hire. Dr. O’Dwyer’s institution received grant support from Ibis Biosciences. Dr. Zacharowski received lecture honoraria from Abbott in the past 3 years and disclosed off-label product use (machine from Abbott). His institution received grant support from Abbott for a clinical trial (Frankfurt was study center and received case money for enrollment of patients. No other payment was received). Dr. Mikaszewska-Sokolewicz disclosed off-label product use (three research assays and three classes of matrices). Her institution received financial support (plane ticked and hotel costs covered for study initiation meeting; hospital was to be paid for study assignment). Dr. Schrenzel received grants from Abbott during the course of the study. Dr. Schrenzel’s institution received grant support. Dr. Simon served as a board member for Beckman Coulter and received grants and personal fees from Ibis Abbott during the conduct of the study. He and his institution consulted for Abbott, bioMérieux, bioRad, and GlaxoSmithKline. He received grant support, support for travel, and support for participation in review activities. Dr. Wilks received support (Abbott paid for installation and running of PlexID platform), disclosed off-label product use (Abbott PlexID now Iridica is CE marked but not the Food and Drug Administration), and received support for article research from Abbott. His institution received grant and funding support from Abbott. His institution received refund of traveling expenses (never claimed, dating back for a couple of years). Dr. Picard-Maureau disclosed off-label product use (product now for diagnostic use in the European Union [CE-In-vitro Diagnostics]) and received funding from Abbott (full-time employee of Abbott and worked on that project as part of job). Dr. Chalfin received funding (employee of Abbott and also received stock grants as part of employment). Dr. Ecker received funding (employee of Abbott that manufactures the technology). Dr. Sampath disclosed relationships (full-time employee of Abbott). Dr. Singer received grant support and funding from Abbott.
Figures
Comment in
-
On the Threshold of a Dream.Crit Care Med. 2015 Nov;43(11):2504-6. doi: 10.1097/CCM.0000000000001323. Crit Care Med. 2015. PMID: 26468701 Free PMC article. No abstract available.
-
Rapid Diagnosis of Infection in Critically Ill: Is Molecular Diagnosis the Magic Bullet?Crit Care Med. 2016 May;44(5):e314-5. doi: 10.1097/CCM.0000000000001549. Crit Care Med. 2016. PMID: 27083038 No abstract available.
-
The authors reply.Crit Care Med. 2016 May;44(5):e315. doi: 10.1097/CCM.0000000000001594. Crit Care Med. 2016. PMID: 27083039 No abstract available.
References
-
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589–1596. - PubMed
-
- Fenollar F, Raoult D. Molecular diagnosis of bloodstream infections caused by non-cultivable bacteria. Int J Antimicrob Agents. 2007;30(Suppl 1):S7–15. - PubMed
-
- Lamy B, Roy P, Carret G, et al. What is the relevance of obtaining multiple blood samples for culture? A comprehensive model to optimize the strategy for diagnosing bacteremia. Clin Infect Dis. 2002;35:842–850. - PubMed
