

Acceptability of Home-Assessment Post Medical Abortion and Medical Abortion in a Low-Resource Setting in Rajasthan, India. Secondary Outcome Analysis of a Non-Inferiority Randomized Controlled Trial
- PMID: 26327217
- PMCID: PMC4556554
- DOI: 10.1371/journal.pone.0133354
Acceptability of Home-Assessment Post Medical Abortion and Medical Abortion in a Low-Resource Setting in Rajasthan, India. Secondary Outcome Analysis of a Non-Inferiority Randomized Controlled Trial
Abstract
Background: Studies evaluating acceptability of simplified follow-up after medical abortion have focused on high-resource or urban settings where telephones, road connections, and modes of transport are available and where women have formal education.
Objective: To investigate women's acceptability of home-assessment of abortion and whether acceptability of medical abortion differs by in-clinic or home-assessment of abortion outcome in a low-resource setting in India.
Design: Secondary outcome of a randomised, controlled, non-inferiority trial.
Setting: Outpatient primary health care clinics in rural and urban Rajasthan, India.
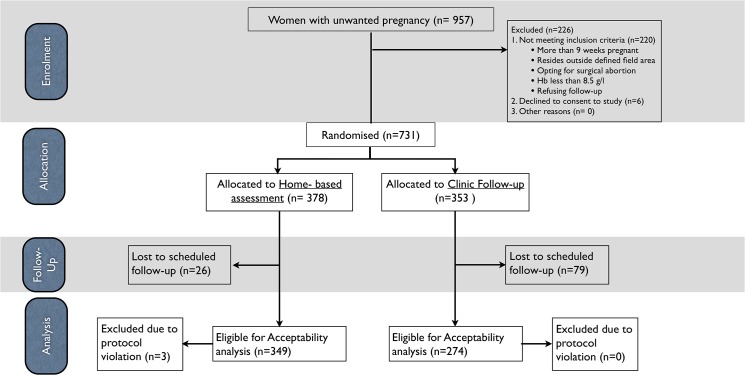
Population: Women were eligible if they sought abortion with a gestation up to 9 weeks, lived within defined study area and agreed to follow-up. Women were ineligible if they had known contraindications to medical abortion, haemoglobin < 85 mg/l and were below 18 years.
Methods: Abortion outcome assessment through routine clinic follow-up by a doctor was compared with home-assessment using a low-sensitivity pregnancy test and a pictorial instruction sheet. A computerized random number generator generated the randomisation sequence (1:1) in blocks of six. Research assistants randomly allocated eligible women who opted for medical abortion (mifepristone and misoprostol), using opaque sealed envelopes. Blinding during outcome assessment was not possible.
Main outcome measures: Women's acceptability of home-assessment was measured as future preference of follow-up. Overall satisfaction, expectations, and comparison with previous abortion experiences were compared between study groups.
Results: 731 women were randomized to the clinic follow-up group (n = 353) or home-assessment group (n = 378). 623 (85%) women were successfully followed up, of those 597 (96%) were satisfied and 592 (95%) found the abortion better or as expected, with no difference between study groups. The majority, 355 (57%) women, preferred home-assessment in the event of a future abortion. Significantly more women, 284 (82%), in the home-assessment group preferred home-assessment in the future, as compared with 188 (70%) of women in the clinic follow-up group, who preferred clinic follow-up in the future (p < 0.001).
Conclusion: Home-assessment is highly acceptable among women in low-resource, and rural, settings. The choice to follow-up an early medical abortion according to women's preference should be offered to foster women's reproductive autonomy.
Trial registration: ClinicalTrials.gov NCT01827995.
Conflict of interest statement
Figures
References
-
- Parliament of the Republic of India: THE MEDICAL TERMINATION OF PREGNANCY AMENDMENT ACT, 2002 (No. 64 of 2002) An Act to amend the Medical Termination of Pregnancy Act, 1971. 2002, 2002:3–5.
-
- Sample Registration System (SRS): SPECIAL BULLETIN ON MATERNAL MORTALITY IN INDIA 2010–12. 2013:1–4.
-
- Hirve SS: Abortion law, policy and services in India: a critical review. Reprod. Health Matters 2004, 12:114–21. - PubMed
-
- National Rural Health Mission, Ministry of Health and Family Welfare, Government of India: Comprehensive Abortion Care—Training and Service Delivery Guidelines New Delhi: Ministry of Health and Family Welfare Government of India; 2010.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
