

Outcomes of Active Surveillance for Clinically Localized Prostate Cancer in the Prospective, Multi-Institutional Canary PASS Cohort
- PMID: 26327354
- PMCID: PMC4970462
- DOI: 10.1016/j.juro.2015.08.087
Outcomes of Active Surveillance for Clinically Localized Prostate Cancer in the Prospective, Multi-Institutional Canary PASS Cohort
Abstract
Purpose: Active surveillance represents a strategy to address the overtreatment of prostate cancer, yet uncertainty regarding individual patient outcomes remains a concern. We evaluated outcomes in a prospective multicenter study of active surveillance.
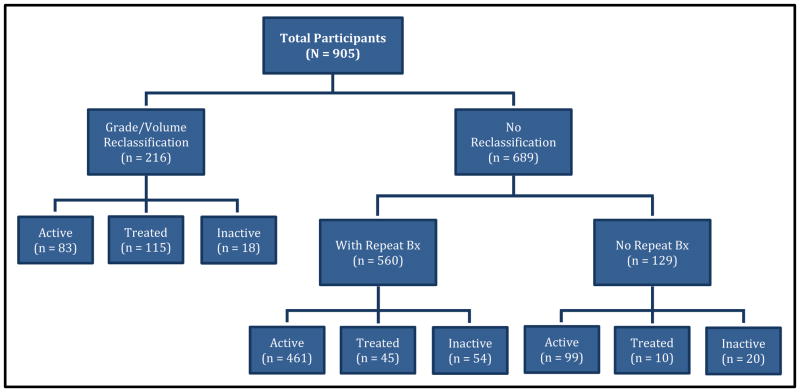
Materials and methods: We studied 905 men in the prospective Canary PASS enrolled between 2008 and 2013. We collected clinical data at study entry and at prespecified intervals, and determined associations with adverse reclassification, defined as increased Gleason grade or greater cancer volume on followup biopsy. We also evaluated the relationships of clinical parameters with pathology findings in participants who underwent surgery after a period of active surveillance.
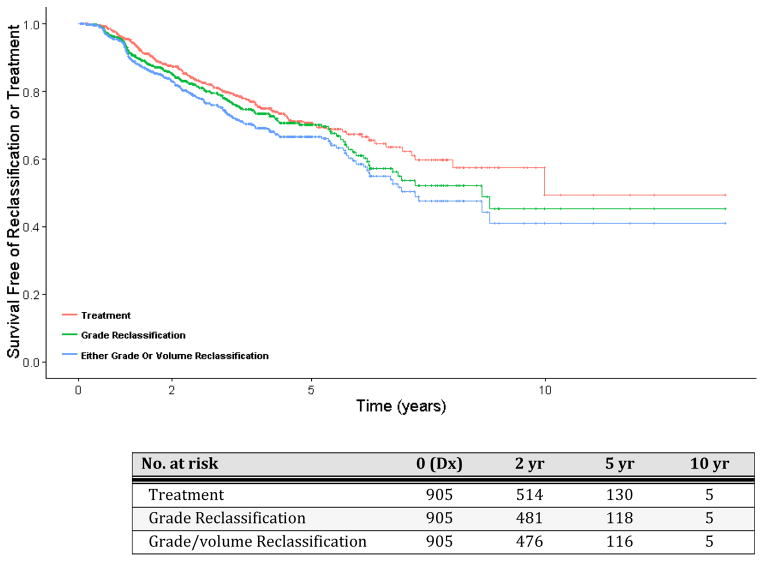
Results: At a median followup of 28 months 24% of participants experienced adverse reclassification, of whom 53% underwent treatment while 31% continued on active surveillance. Overall 19% of participants received treatment, 68% with adverse reclassification, while 32% opted for treatment without disease reclassification. In multivariate Cox proportional hazards modeling the percent of biopsy cores with cancer, body mass index and prostate specific antigen density were associated with adverse reclassification (p=0.01, 0.04, 0.04, respectively). Of 103 participants subsequently treated with radical prostatectomy 34% had adverse pathology, defined as primary pattern 4-5 or nonorgan confined disease, including 2 with positive lymph nodes, with no significant relationship between risk category at diagnosis and findings at surgery (p=0.76).
Conclusions: Most men remain on active surveillance at 5 years without adverse reclassification or adverse pathology at surgery. However, clinical factors had only a modest association with disease reclassification, supporting the need for approaches that improve the prediction of this outcome.
Keywords: prospective studies; prostatic neoplasms; watchful waiting.
Copyright © 2016 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Albertsen PC, Hanley JA, Fine J. 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA. 2005;293(17):2095–2101. - PubMed
-
- Etzioni R, Penson DF, Legler JM, et al. Overdiagnosis due to prostate-specific antigen screening: lessons from U.S. prostate cancer incidence trends. J Natl Cancer Inst. 2002;94(13):981–990. - PubMed
-
- Miller DC, Gruber SB, Hollenbeck BK, et al. Incidence of initial local therapy among men with lower-risk prostate cancer in the United States. J Natl Cancer Inst. 2006;98(16):1134–1141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
