

High Risk of Diabetes and Neurobehavioral Deficits in Individuals With Surgically Treated Hyperinsulinism
- PMID: 26327482
- PMCID: PMC4702456
- DOI: 10.1210/jc.2015-2539
High Risk of Diabetes and Neurobehavioral Deficits in Individuals With Surgically Treated Hyperinsulinism
Abstract
Context: Children with the most common and severe type of congenital hyperinsulinism (HI) frequently require pancreatectomy to control the hypoglycemia. Pancreatectomy increases the risk for diabetes, whereas recurrent hypoglycemia places children at risk of neurocognitive dysfunction. The prevalence of these complications is not well defined.
Objective: The objective was to determine the prevalence of diabetes and neurobehavioral deficits in surgically treated HI.
Design: This was designed as a cross-sectional study of individuals who underwent pancreatectomy for HI between 1960 and 2008.
Outcomes: Diabetes outcomes were assessed through patient interview and medical record review. Neurobehavioral outcomes were assessed through the Adaptive Behavior Assessment System, 2nd edition (ABAS-II), and the Child Behavior Checklist (CBCL).
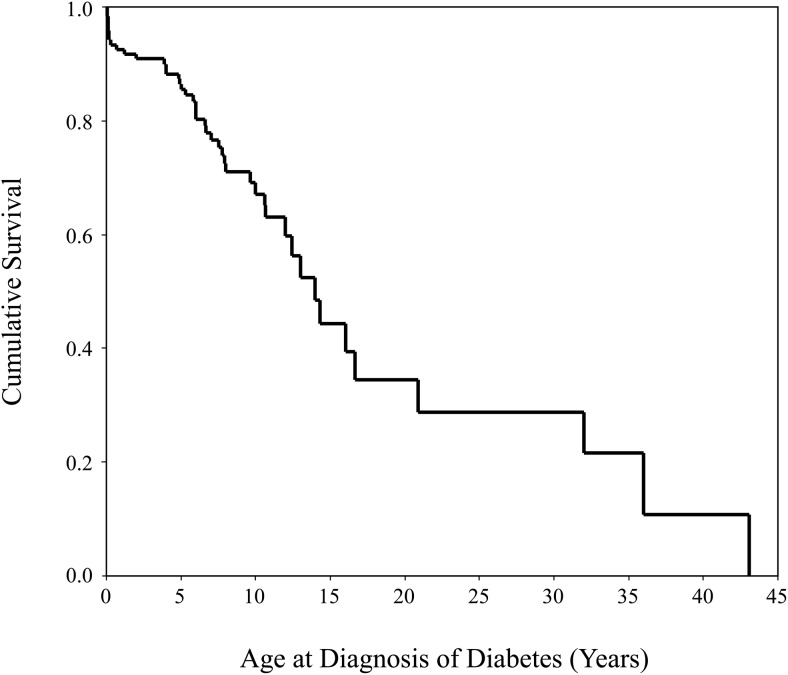
Results: A total of 121 subjects were enrolled in the study at a median age of 8.9 years (range, 3.5-50.7 y). Thirty-six percent (44 of 121) of subjects had diabetes. Nine subjects developed diabetes immediately after pancreatectomy. Of the remaining 35 subjects who developed diabetes, the median age at diabetes diagnosis was 7.7 years (range, 8 mo to 43 y). In subjects with diabetes, the median hemoglobin A1c was 7.4% (range, 6.5-12.6%), and 38 (86%) subjects required insulin. Subjects with diabetes had a greater percentage of pancreatectomy than subjects without diabetes (95% [range, 65-98] vs 65% [1-98]). Neurobehavioral abnormalities were reported in 58 (48%) subjects. Nineteen (28%) subjects had abnormal ABAS-II scores, and 10 (16%) subjects had abnormal CBCL scores.
Conclusions: Children, who undergo near-total pancreatectomy are at high risk of developing diabetes. Neurobehavioral deficits are common, and developmental assessment is essential for children with HI.
Figures
References
-
- Thomas PM, Cote GJ, Wohllk N, et al. Mutations in the sulfonylurea receptor gene in familial persistent hyperinsulinemic hypoglycemia of infancy. Science. 1995;268:426–429. - PubMed
-
- Thomas P, Ye Y, Lightner E. Mutation of the pancreatic islet inward rectifier Kir6.2 also leads to familial persistent hyperinsulinemic hypoglycemia of infancy. Hum Mol Genet. 1996;5:1809–1812. - PubMed
-
- De Leon DD, Stanley CA. Pathophysiology of diffuse ATP-sensitive potassium channel hyperinsulinism. In: Stanley CA, De Leon DD, eds. Monogenic Hyperinsulinemic Hypoglycemia Disorders. 1st ed Vol 21 Basel, Switzerland: Karger; 2012:18–29.
-
- Rahier J, Fält K, Müntefering H, Becker K, Gepts W, Falkmer S. The basic structural lesion of persistent neonatal hypoglycaemia with hyperinsulinism: deficiency of pancreatic D cells or hyperactivity of B cells? Diabetologia. 1984;26:282–289. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
