

Evidence of High Out of Pocket Spending for HIV Care Leading to Catastrophic Expenditure for Affected Patients in Lao People's Democratic Republic
- PMID: 26327558
- PMCID: PMC4556637
- DOI: 10.1371/journal.pone.0136664
Evidence of High Out of Pocket Spending for HIV Care Leading to Catastrophic Expenditure for Affected Patients in Lao People's Democratic Republic
Abstract
Background: The scaling up of antiviral treatment (ART) coverage in the past decade has increased access to care for numerous people living with HIV/AIDS (PLWHA) in low-resource settings. Out-of-pocket payments (OOPs) represent a barrier for healthcare access, adherence and ART effectiveness, and can be economically catastrophic for PLWHA and their family. We evaluated OOPs of PLWHA attending outpatient and inpatient care units and estimated the financial burden for their households in the Lao People's Democratic Republic. We assumed that such OOPs may result in catastrophic health expenses in this context with fragile economical balance and low health insurance coverage.
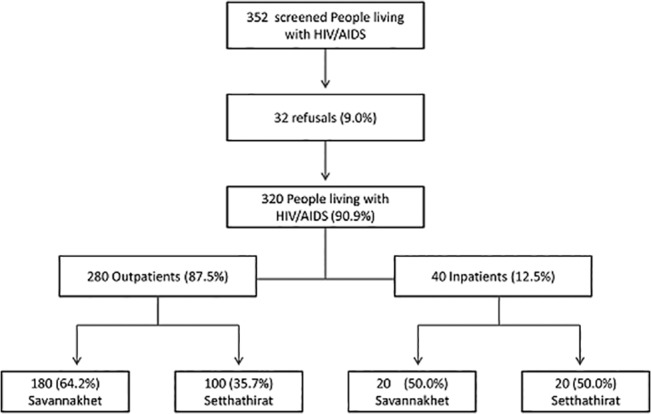
Methods: We conducted a cross-sectional survey of a randomized sample of routine outpatients and a prospective survey of consecutive new inpatients at two referral hospitals (Setthathirat in the capital city, Savannaket in the province). After obtaining informed consent, PLWHA were interviewed using a standardized 82-item questionnaire including information on socio-economic characteristics, disease history and coping strategies. All OOPs occurring during a routine visit or a hospital stay were recorded. Household capacity-to-pay (overall income minus essential expenses), direct and indirect OOPs, OOPs per outpatient visit and per inpatient stay as well as catastrophic spending (greater than or equal to 40% of the capacity-to-pay) were calculated. A multivariate analysis of factors associated with catastrophic spending was conducted.
Results: A total of 320 PLWHA [280 inpatients and 40 outpatients; 132 (41.2%) defined as poor, and 269 (84.1%) on ART] were enrolled. Monthly median household income, essential expenses and capacity-to-pay were US$147.0 (IQR: 86-242), $126 (IQR: 82-192) and $14 (IQR: 19-80), respectively. At the provincial hospital OOPs were higher during routine visits, but three fold lower during hospitalization than in the central hospital ($21.0 versus $18.5 and $110.8 versus $329.8 respectively (p<0.01). The most notable OOPs were related to transportation and to loss of income. A total of 150 patients (46.8%; 95%CI: 41.3-52.5) were affected by catastrophic health expenses; 36 outpatients (90.0%; 95%CI: 76.3-97.2) and 114 inpatients (40.7%; 95%CI: 34.9-46.7). A total of 141 (44.0%) patients had contracted loans, and 127 (39.6%) had to sell some of their assets. In the multivariate analysis, being of Lao Loum ethnic group (Coef.-1.4; p = 0.04); being poor (Coef. -1.0; p = 0.01) and living more than 100 km away from the hospital (Coef.-1.0; p = 0.002) were positively associated with catastrophic spending. Conversely being in the highest wealth quartile (Coef. 1.6; p<0.001), living alone (Coef. 1.1; p = 0.04), attending the provincial hospital (Coef. 1.0; p = 0.002), and being on ART (Coef.1.2; p = 0.003), were negatively associated with catastrophic spending.
Conclusion: PLWHA's households face catastrophic OOPs that are not directly attributable to the cost of ART or to follow-up tests, particularly during a hospitalization period. Transportation, distance to healthcare and time spent at the health facility are the major contributors for OOPs and for indirect opportunity costs. Being on ART and attending the provincial hospital were associated with a lower risk of catastrophic spending. Decentralization of care, access to ART and alleviation of OOPs are crucial factors to successfully decrease the household burden of HIV-AIDS expenses.
Conflict of interest statement
References
-
- Tran BX, Duong AT, Nguyen LT, Hwang J, Nguyen BT, Nguyen QT, et al. (2013) Financial burden of health care for HIV/AIDS patients in Vietnam. Tropical Medicine & International Health 18: 212–218. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
