

Review
doi: 10.1055/s-0035-1556878.
Surveillance Imaging Following Endovascular Aneurysm Repair
Affiliations
- PMID: 26327742
- PMCID: PMC4540620
- DOI: 10.1055/s-0035-1556878
Item in Clipboard
Review
Surveillance Imaging Following Endovascular Aneurysm Repair
Semin Intervent Radiol.
2015 Sep.
Abstract
There is a significant risk of complication following endovascular abdominal repair (EVAR), including endoleak, graft translocation, thrombosis, and infection. Surveillance imaging is important for detecting EVAR complication. Surveillance modalities include conventional X-ray, computed tomography, magnetic resonance imaging, ultrasound, and conventional angiography, with inherent advantages and drawbacks to each modality. The authors present common complications following EVAR, and recent advances in the key modalities for surveillance.
Keywords: abdominal aortic aneurysm; endoleak; endovascular aneurysm repair; interventional radiology; surveillance imaging.
Figures
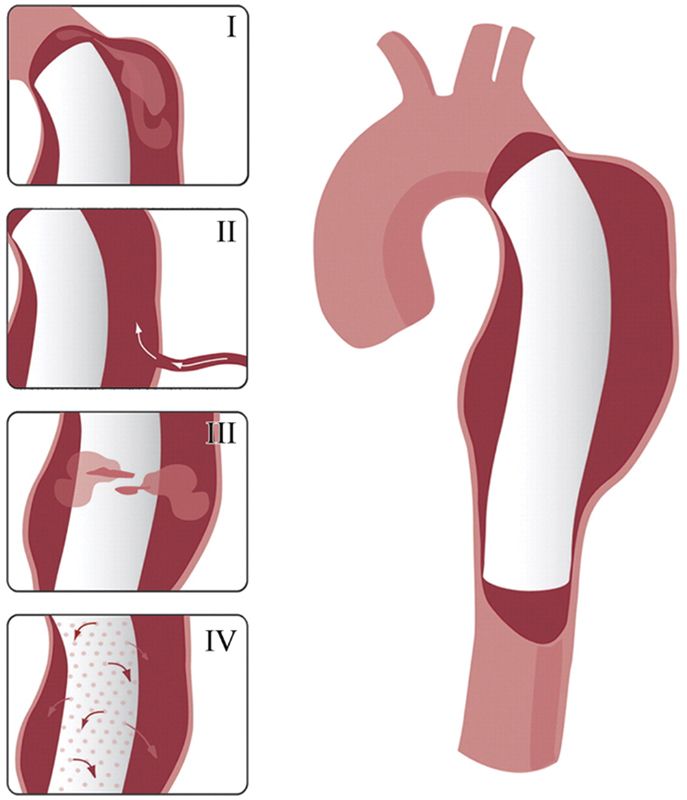
Drawings illustrating the various types of endoleak: type I, attachment site; type II, collateral vessel; type III, graft failure, type IV, graft porosity. (Reprinted with permission from Agarwal P et al. Multidetector CT of thoracic aortic aneurysms. Radiographics 2009; 29:537–552).
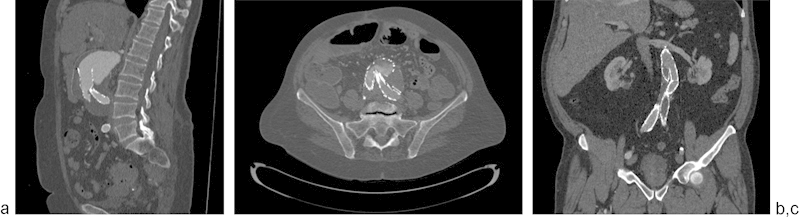
(a) Graft migration with type 1 endoleak (arrow), (b) graft kinking with turbulent flow in lumen, (c) graft kinking with thrombosis of left iliac limb (arrow).

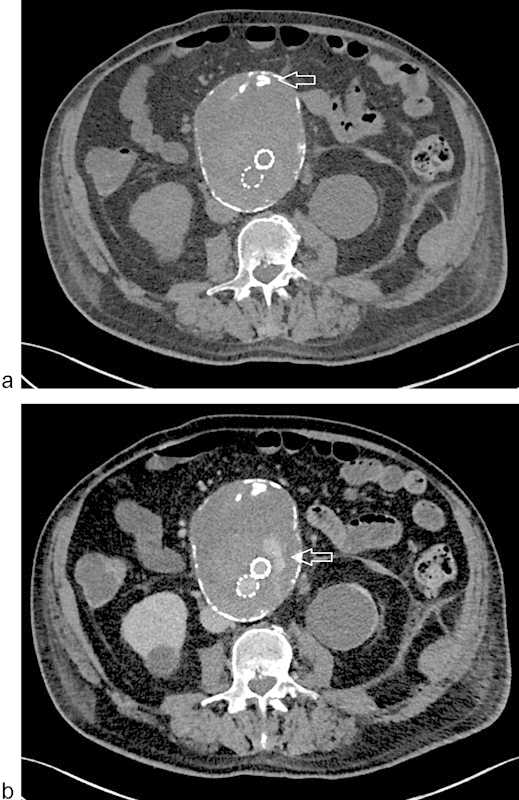
(a) Graft infection with air in the sac (arrow); (b) graft infection with aorto-ureteric fistula and pyelonephritis.
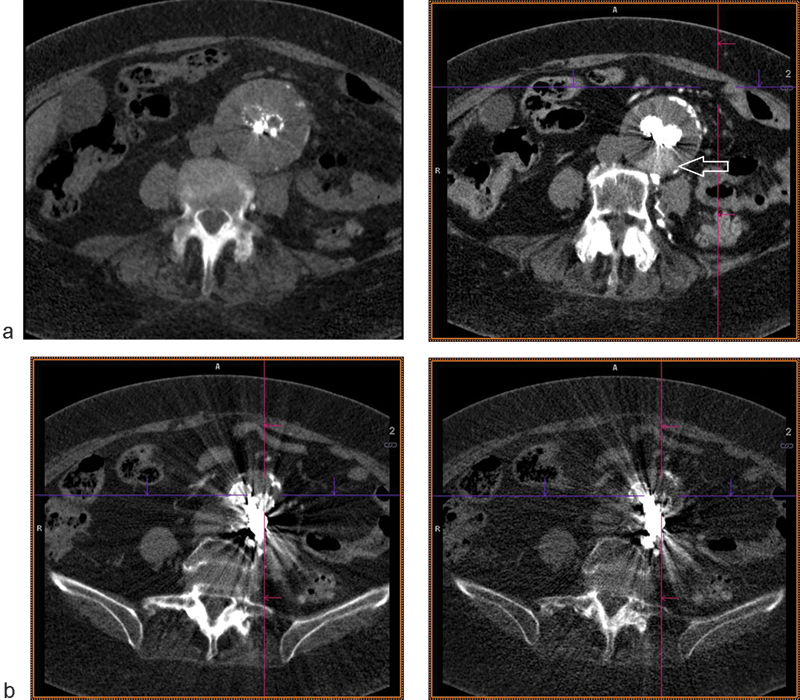
CTA of EVAR. (a) Misleading high attenuation due to neointimal calcium seen on unenhanced imaging (arrow); (b) true endoleak revealed on delayed imaging (arrow).
DE-CTA of EVAR. (a) Dose saving from virtual unenhanced reconstruction shown on left; posterior endoleak shown on delayed image on right (arrow). (b) Reduction in coil photon attenuation with monoenergetic beam reconstruction at low (left) and high (right) keV settings.
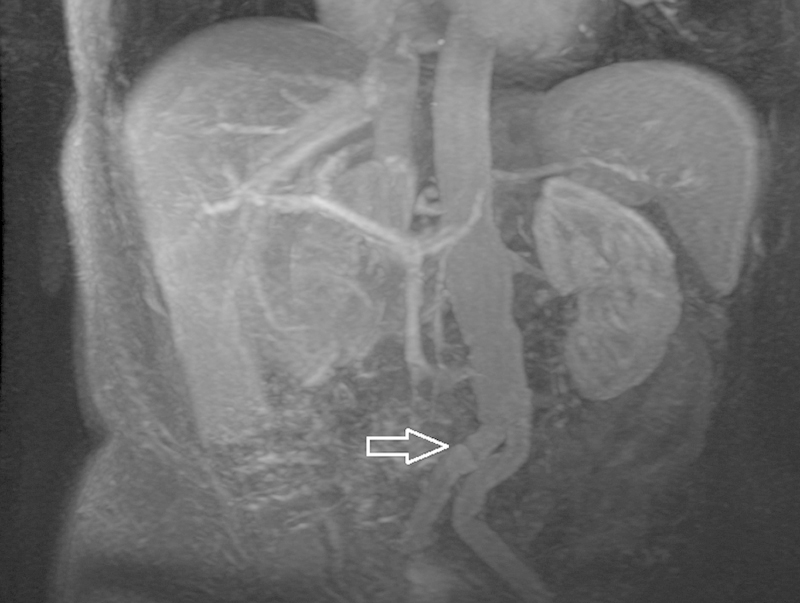
MRA maximum intensity projection of EVAR showing kinking in the iliac limbs (arrow).

Conventional angiography of EVAR. (a) Previously embolized endoleak via translumbar approach shows residual type 2 endoleak supplied via the IMA (circle), here injected through the marginal artery from an SMA approach; (b) successful coil embolization of the IMA with resolution of endoleak (arrow).
Similar articles
-
Surveillance Imaging following Endovascular Aneurysm Repair: State of the Art.Semin Intervent Radiol. 2020 Oct;37(4):356-364. doi: 10.1055/s-0040-1715882. Epub 2020 Oct 1. Semin Intervent Radiol. 2020. PMID: 33041481 Free PMC article. Review.
-
Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management.Cardiovasc Diagn Ther. 2018 Apr;8(Suppl 1):S138-S156. doi: 10.21037/cdt.2017.09.17. Cardiovasc Diagn Ther. 2018. PMID: 29850426 Free PMC article. Review.
-
Evaluating outcomes of endoleak discrepancies between computed tomography scan and ultrasound imaging after endovascular abdominal aneurysm repair.Ann Vasc Surg. 2011 Jan;25(1):94-100. doi: 10.1016/j.avsg.2010.08.003. Ann Vasc Surg. 2011. PMID: 21172584
-
Defining a role for contrast-enhanced ultrasound in endovascular aneurysm repair surveillance.J Vasc Surg. 2013 Jul;58(1):18-23. doi: 10.1016/j.jvs.2012.12.057. Epub 2013 Mar 13. J Vasc Surg. 2013. PMID: 23490295
-
Redefining postoperative surveillance after endovascular aneurysm repair: recommendations based on 5-year follow-up in the US Zenith multicenter trial.J Vasc Surg. 2008 Aug;48(2):278-84; discussion 284-5. doi: 10.1016/j.jvs.2008.02.075. Epub 2008 Jun 24. J Vasc Surg. 2008. PMID: 18572368
Cited by
-
Status of diagnosis and therapy of abdominal aortic aneurysms.Front Cardiovasc Med. 2023 Jul 28;10:1199804. doi: 10.3389/fcvm.2023.1199804. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37576107 Free PMC article. Review.
-
Dynamic Radial MR Imaging for Endoleak Surveillance after Endovascular Repair of Abdominal Aortic Aneurysms with Inconclusive CT Angiography: A Prospective Study.J Clin Med. 2024 May 15;13(10):2913. doi: 10.3390/jcm13102913. J Clin Med. 2024. PMID: 38792455 Free PMC article.
-
Individualizing Surveillance after Endovascular Aortic Repair Using a Modular Imaging Algorithm.Diagnostics (Basel). 2024 Apr 29;14(9):930. doi: 10.3390/diagnostics14090930. Diagnostics (Basel). 2024. PMID: 38732344 Free PMC article.
-
Left Renal Artery Chronic Occlusion in the Setting of Extensive Intraprosthetic Mural Thrombus in an Abdominal Aortic Endograft.Cureus. 2024 May 4;16(5):e59624. doi: 10.7759/cureus.59624. eCollection 2024 May. Cureus. 2024. PMID: 38832185 Free PMC article.
-
Abdominal aneurysm sac thrombus CT density and volume after EVAR: which association with underlying endoleak?Eur Radiol Exp. 2024 Aug 1;8(1):88. doi: 10.1186/s41747-024-00489-3. Eur Radiol Exp. 2024. PMID: 39090441 Free PMC article.
References
-
- Singh K, Bønaa K H, Jacobsen B K, Bjørk L, Solberg S. Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study: The Tromsø Study. Am J Epidemiol. 2001;154(3):236–244. - PubMed
-
- McPhee J T, Hill J S, Eslami M H. The impact of gender on presentation, therapy, and mortality of abdominal aortic aneurysm in the United States, 2001-2004. J Vasc Surg. 2007;45(5):891–899. - PubMed
-
- Parodi J C, Palmaz J C, Barone H D. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann Vasc Surg. 1991;5(6):491–499. - PubMed
-
- Greenhalgh R M Brown L C Kwong G P Powell J T Thompson S G; EVAR trial participants. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial Lancet 20043649437843–848. - PubMed
-
- Schermerhorn M L, O'Malley A J, Jhaveri A, Cotterill P, Pomposelli F, Landon B E. Endovascular vs. open repair of abdominal aortic aneurysms in the Medicare population. N Engl J Med. 2008;358(5):464–474. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
