

Emergent Endovascular Stent Grafts for Ruptured Aortic Aneurysms
- PMID: 26327743
- PMCID: PMC4540621
- DOI: 10.1055/s-0035-1556879
Emergent Endovascular Stent Grafts for Ruptured Aortic Aneurysms
Abstract
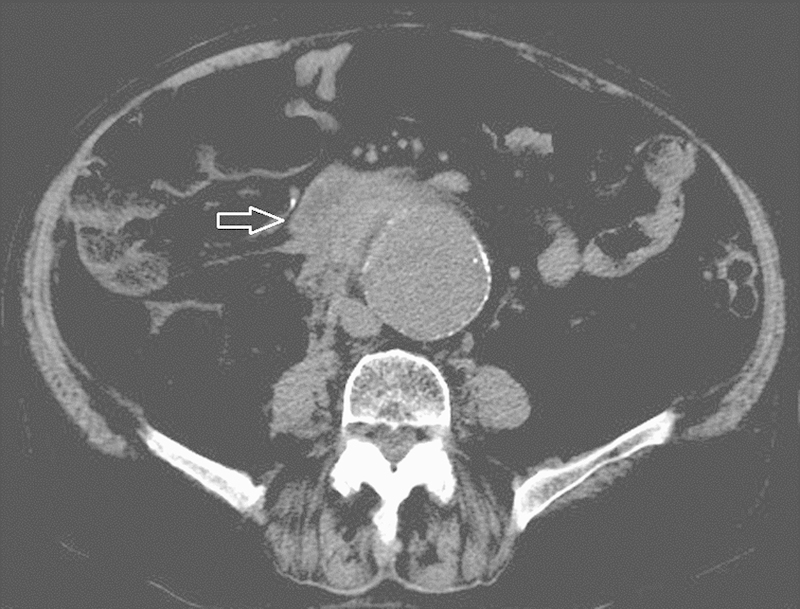
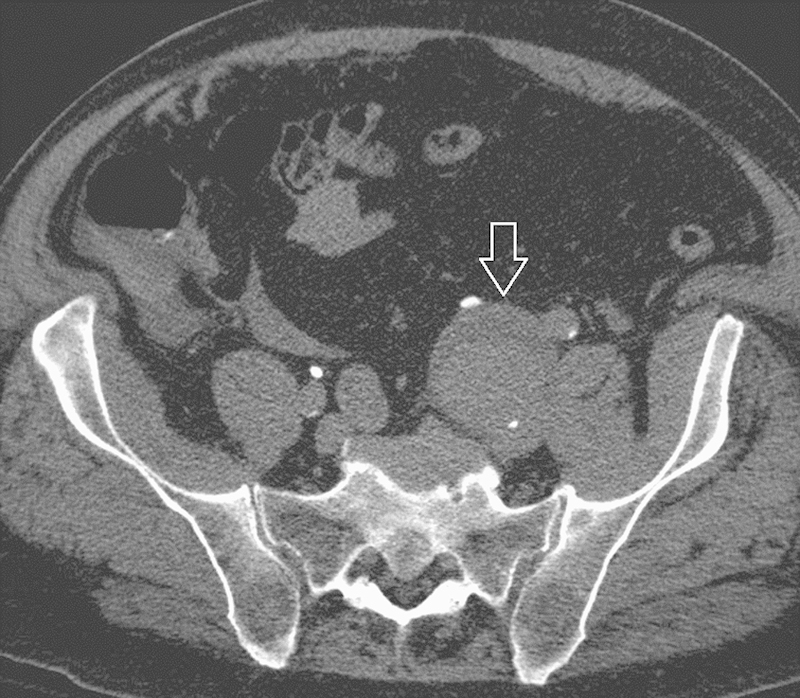
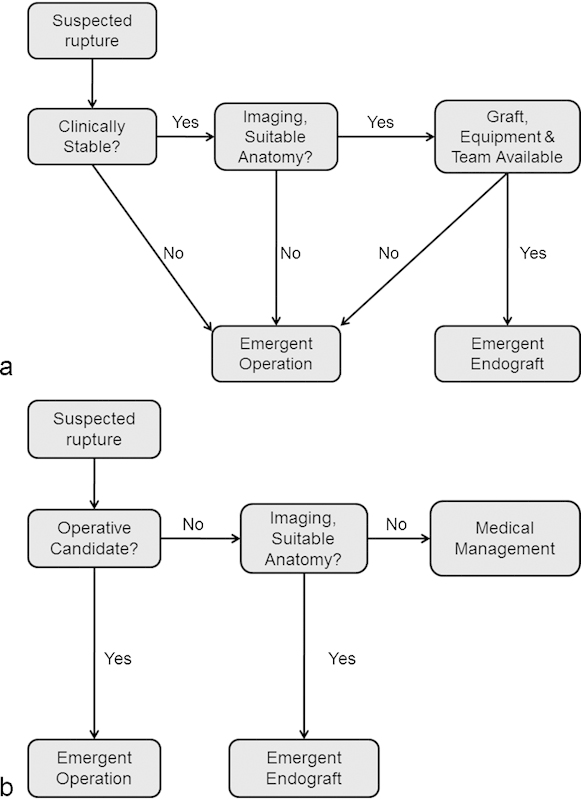
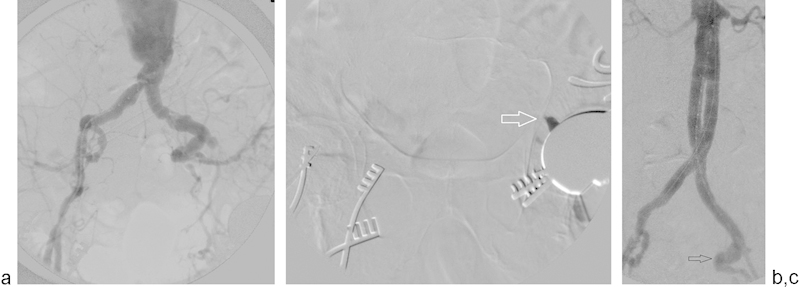
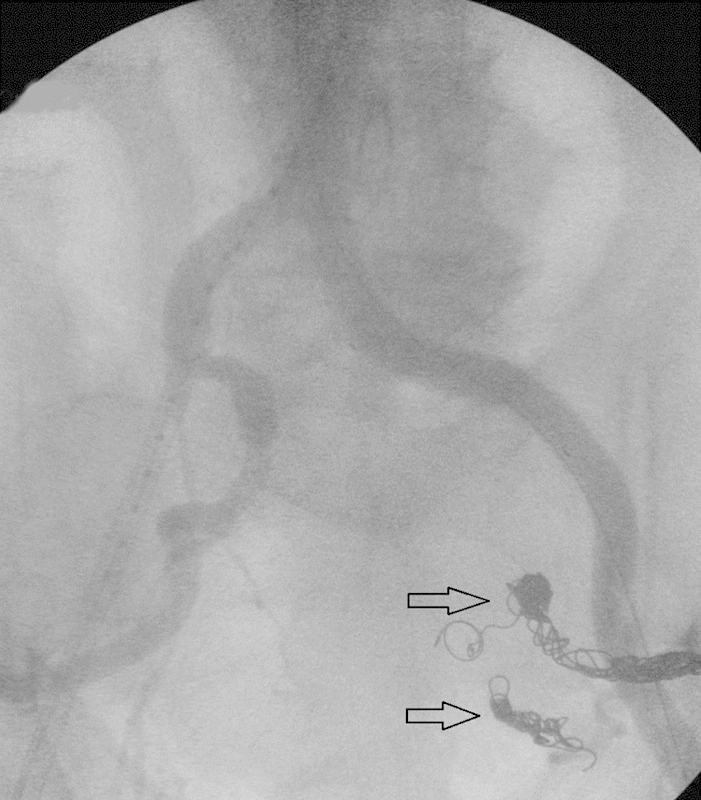
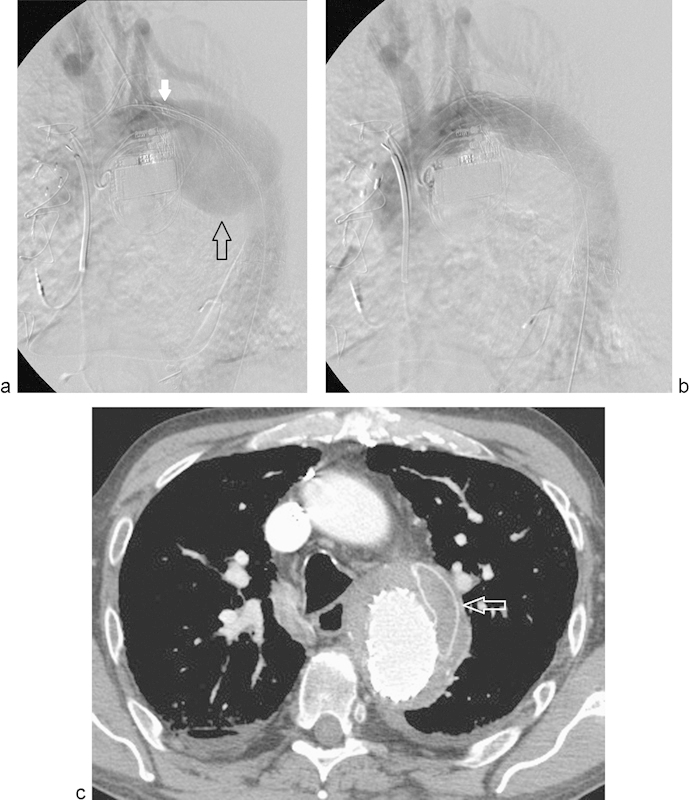
Ruptured aortic aneurysms uniformly require emergent attention. Historically, urgent surgical repair or medical management was the only treatment options. The development of covered stent grafts has introduced a third approach in the care of these critical patients. The clinical status of the patient and local physician expertise drive the treatment modalities in the majority of cases. The goal of therapy in these patients is to stabilize the patient as quickly as possible, establish maximum survival with minimum morbidity, and provide a long lasting result. The endovascular approach has become an acceptable treatment option in an increasing number of patients presenting with ruptured aneurysmal disease of both the descending thoracic and abdominal aorta. Major factors influencing treatment include patient clinical status, characteristics of the aorta, physician preference, institutional experience, and availability of appropriate equipment. Planning, experience, and the ability to improvise effective solutions are keys to the success of the procedure when endovascular techniques are utilized. Three separate cases, requiring intraprocedural improvisation, are presented followed by a review of the literature.
Keywords: EVAR; TEVAR; emergent stent graft; interventional radiology; ruptured aneurysm.
Figures

References
-
- Greenhalgh R M Brown L C Kwong G P Powell J T Thompson S G; EVAR trial participants. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial Lancet 20043649437843–848. - PubMed
-
- Prinssen M, Verhoeven E L, Buth J. et al. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004;351(16):1607–1618. - PubMed
-
- Fairman R M, Criado F, Farber M. et al. Pivotal results of the Medtronic Vascular Talent Thoracic Stent Graft System: the VALOR trial. J Vasc Surg. 2008;48(3):546–554. - PubMed
-
- Makaroun M S Dillavou E D Wheatley G H Cambria R P; Gore TAG Investigators. Five-year results of endovascular treatment with the Gore TAG device compared with open repair of thoracic aortic aneurysms J Vasc Surg 2008475912–918. - PubMed
-
- Matsumura J S Cambria R P Dake M D Moore R D Svensson L G Snyder S; TX2 Clinical Trial Investigators. International controlled clinical trial of thoracic endovascular aneurysm repair with the Zenith TX2 endovascular graft: 1-year results J Vasc Surg 2008472247–257., discussion 257 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
