

Current Status of Percutaneous Endografting
- PMID: 26327747
- PMCID: PMC4540623
- DOI: 10.1055/s-0035-1556826
Current Status of Percutaneous Endografting
Abstract
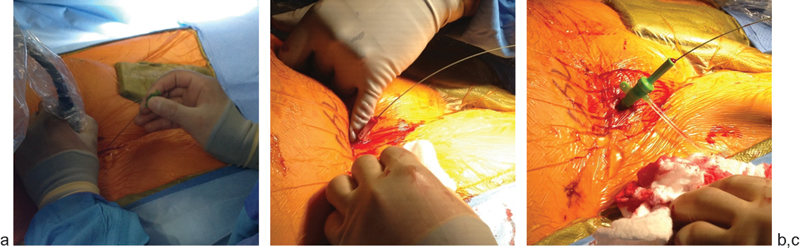
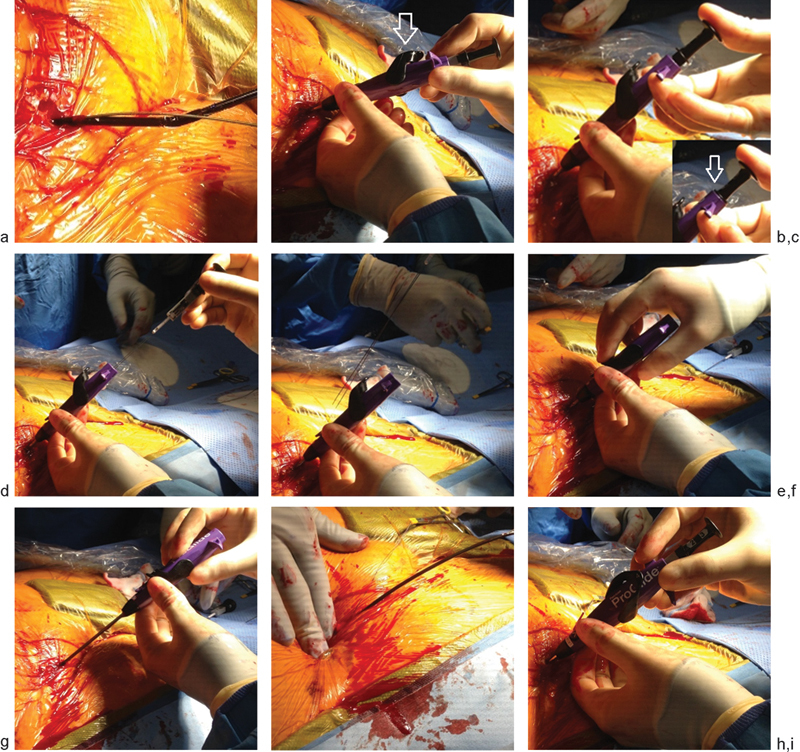
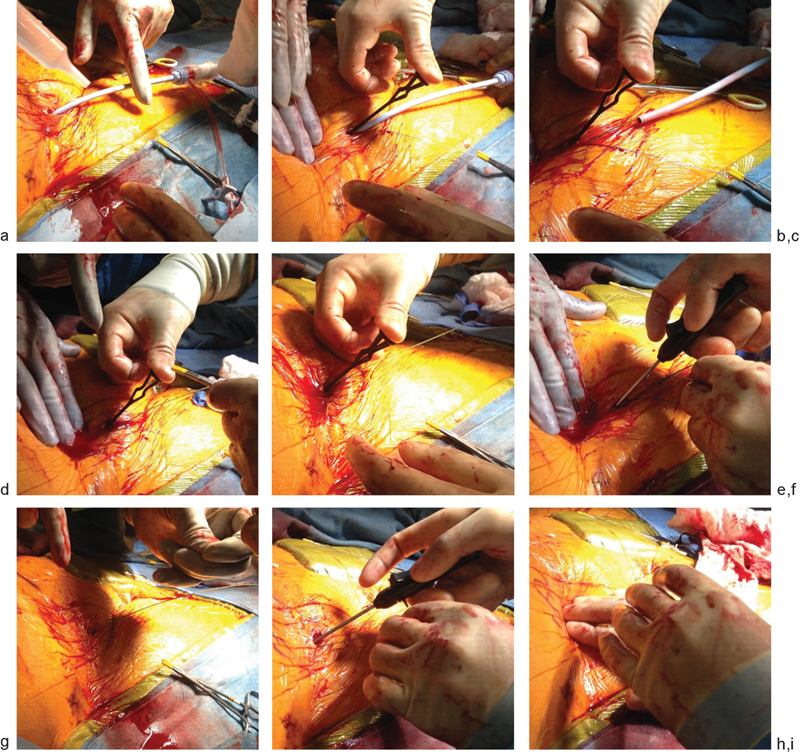
Totally percutaneous endovascular abdominal aortic aneurysm repair (PEVAR) using suture-mediated closure devices (SMCDs) has several well-established advantages over standard open femoral exposure as a direct consequence of being less invasive and having shorter times to hemostasis and procedure completion. The first multicenter randomized controlled trial designed to assess the safety and efficacy of PEVAR and to compare percutaneous access with standard open femoral exposure was recently published (the PEVAR trial). The PEVAR trial demonstrated that percutaneous endografting is safe, effective, and noninferior to standard open femoral exposure among trained operators. The study reaffirmed the results of several recent single center and nonrandomized studies, demonstrating that percutaneous access facilitated shorter procedures, shorter times to secure hemostasis, and improved quality of life for patients. As PEVAR has gained popularity among patients and physicians, refinements to the technique and patient selection process have been made. There has been growing interest in treating patients with anatomical characteristics previously thought to be unsuitable for PEVAR, such as common femoral artery (CFA) calcifications, scarred groins, small CFA diameter, and high patient body mass index (BMI). However, observance of strict procedural technique and consideration for patient selection criteria remain paramount in achieving acceptable technical success rates with PEVAR.
Keywords: PEVAR; ProGlide; interventional radiology; preclose.
Figures

References
-
- Nelson P R, Kracjer Z, Kansal N. et al. A multicenter, randomized, controlled trial of totally percutaneous access versus open femoral exposure for endovascular aortic aneurysm repair (the PEVAR trial) J Vasc Surg. 2014;59(5):1181–1193. - PubMed
-
- Haas P C, Krajcer Z, Diethrich E B. Closure of large percutaneous access sites using the Prostar XL Percutaneous Vascular Surgery device. J Endovasc Surg. 1999;6(2):168–170. - PubMed
-
- Dosluoglu H H, Cherr G S, Harris L M, Dryjski M L. Total percutaneous endovascular repair of abdominal aortic aneurysms using Perclose ProGlide closure devices. J Endovasc Ther. 2007;14(2):184–188. - PubMed
-
- Torsello G B, Kasprzak B, Klenk E, Tessarek J, Osada N, Torsello G F. Endovascular suture versus cutdown for endovascular aneurysm repair: a prospective randomized pilot study. J Vasc Surg. 2003;38(1):78–82. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
