

Non-functional neuroendocrine tumors of the pancreas: Advances in diagnosis and management
- PMID: 26327759
- PMCID: PMC4548112
- DOI: 10.3748/wjg.v21.i32.9512
Non-functional neuroendocrine tumors of the pancreas: Advances in diagnosis and management
Abstract
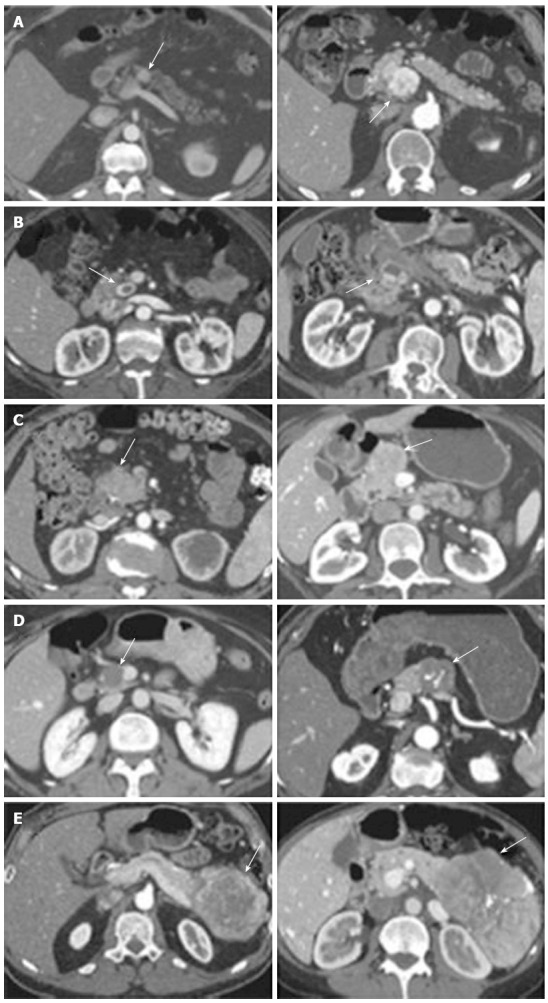
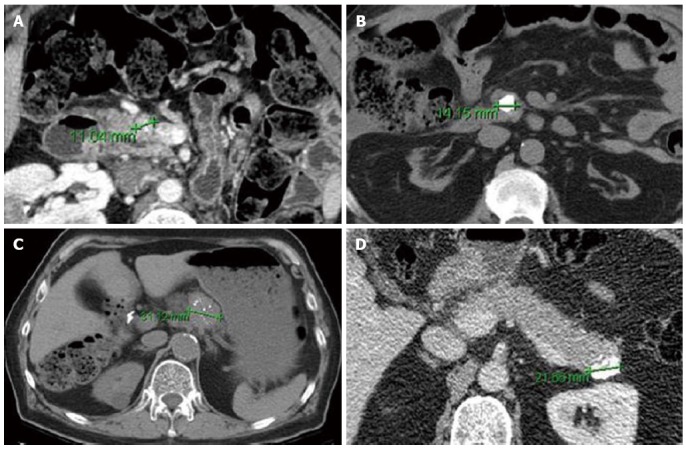
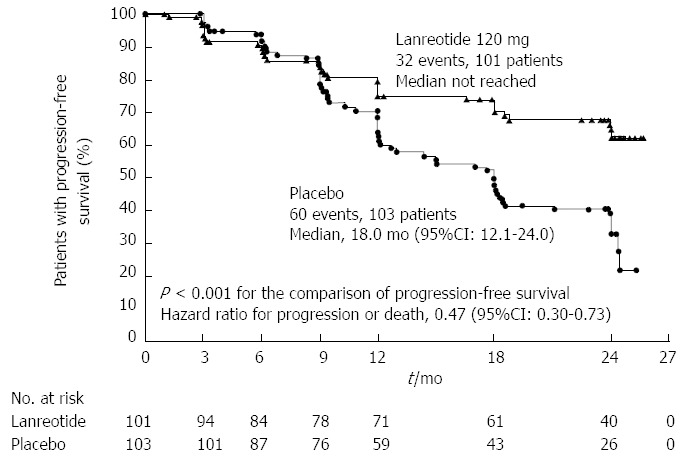
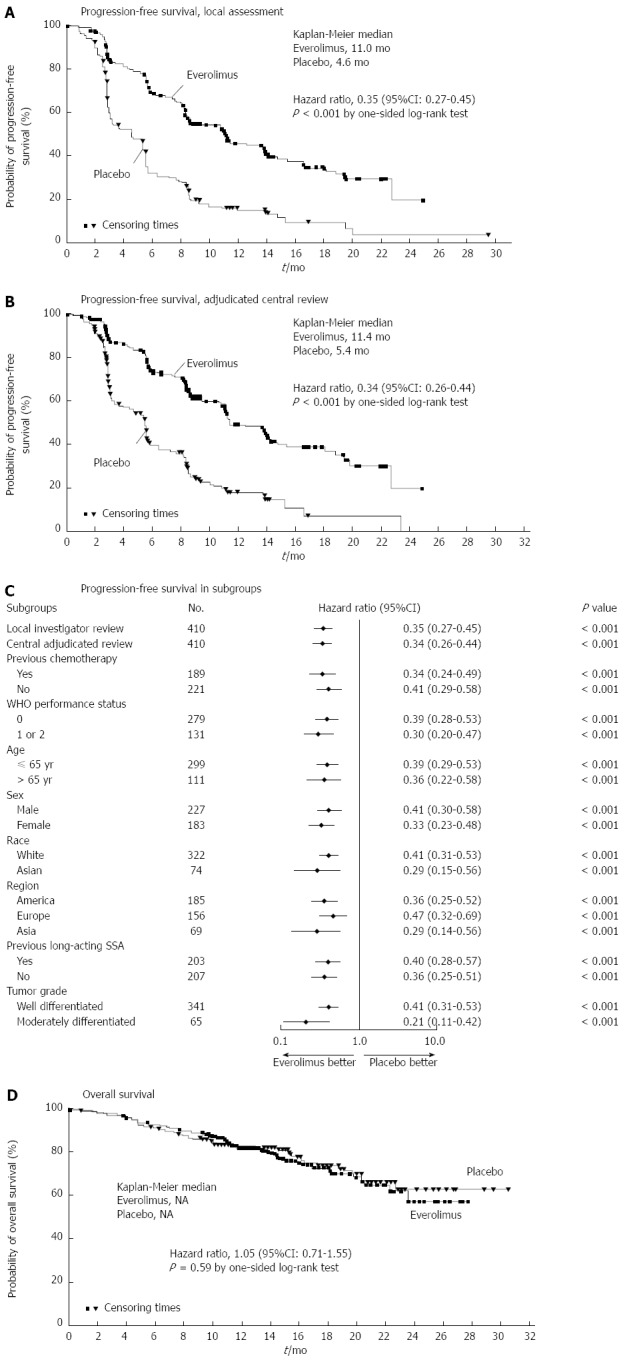
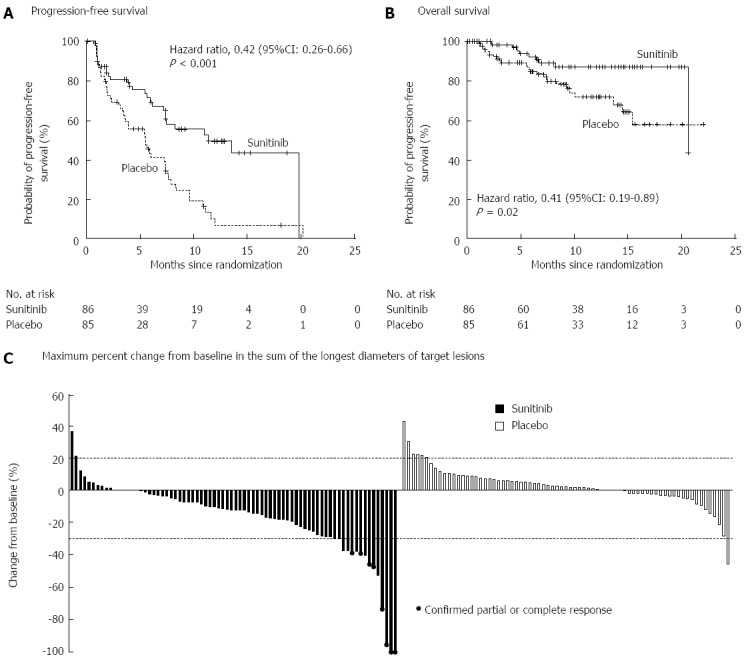
Nonfunctional neuroendocrine tumors of the pancreas (NF-PNETs) are a heterogeneous group of neoplasms. Although rare, the incidence of NF-PNETs is increasing significantly. The classification of PNETs has evolved over the past decades and is now based on a proliferation grading system. While most NF-PNETs are slow growing, tumors with more aggressive biology may become incurable once they progress to unresectable metastatic disease. Tumors of higher grade can be suspected preoperatively based on the presence of calcifications, hypoenhancement on arterial phase computed tomography, positron emission technology avidity and lack of octreotide scan uptake. Surgery is the only curative treatment and is recommended for most patients for whom complete resection is possible. Liver-directed therapies (thermal ablation, transarterial embolization) can be useful in controlling unresectable hepatic metastatic disease. In the presence of unresectable progressive disease, somatostatin analogues, everolimus and sunitinib can prolong progression-free survival. This article provides a comprehensive review of NF-PNETs with special emphasis on recent advances in diagnosis and management.
Keywords: Islet cell; Neuroendocrine carcinoma; Neuroendocrine tumor; Octreotide; Pancreas.
Figures
References
-
- Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin North Am. 2011;40:1–18, vii. - PubMed
-
- Hallet J, Law CH, Cukier M, Saskin R, Liu N, Singh S. Exploring the rising incidence of neuroendocrine tumors: a population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer. 2015;121:589–597. - PubMed
-
- Kimura W, Kuroda A, Morioka Y. Clinical pathology of endocrine tumors of the pancreas. Analysis of autopsy cases. Dig Dis Sci. 1991;36:933–942. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
