

Vaginal hysterectomy vs. laparoscopically assisted vaginal hysterectomy in women with symptomatic uterine leiomyomas: a retrospective study
- PMID: 26327861
- PMCID: PMC4520370
- DOI: 10.5114/pm.2014.45000
Vaginal hysterectomy vs. laparoscopically assisted vaginal hysterectomy in women with symptomatic uterine leiomyomas: a retrospective study
Abstract
Introduction: Uterine leiomyomas are the most common benign tumors of the female reproductive system. Although the majority of myomas are asymptomatic, some patients have symptoms or signs of varying degrees and require a hysterectomy.
The aim of the study: The aim of the study was to compare the clinical results of two minimally invasive hysterectomy techniques: vaginal hysterectomy (VH) and laparoscopically assisted vaginal hysterectomy (LAVH).
Material and methods: A retrospective, observational study was performed at a tertiary care center: the Gynecology and Gynecologic Oncology Department, Polish Mother's Memorial Hospital Research Institute. The study period was from January 2003 to December 2012. A total of 159 women underwent either vaginal hysterectomy (VH, n = 120) or laparoscopically assisted vaginal hysterectomy (LAVH, n = 39) for symptomatic uterine myomas. Outcome measures, including past medical history, blood loss, major complications, operating time and discharge time were assessed and compared between the studied groups. Statistical analysis was performed using Student t-test, U-Mann Whitney test, χ(2) test and Yates'χ(2) test. P < 0.05 was considered statistically significant.
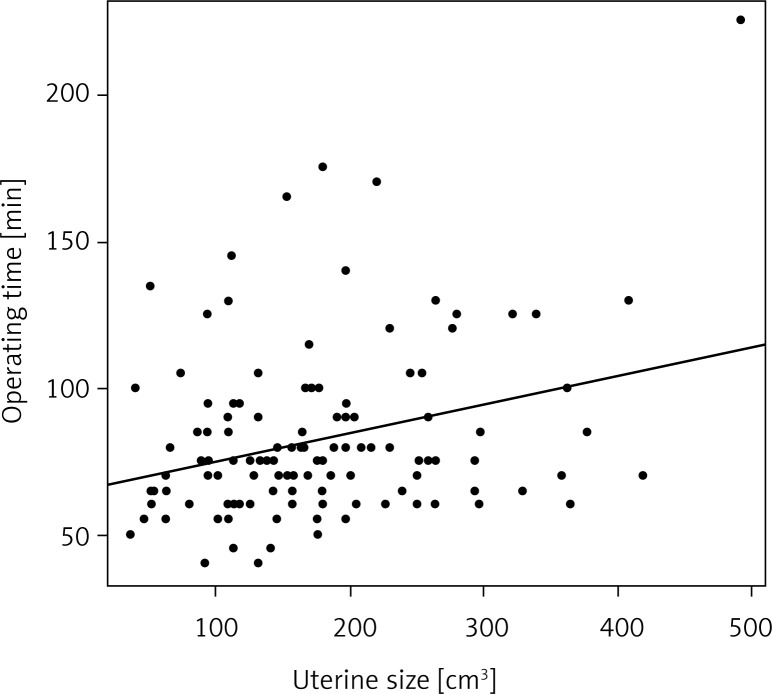
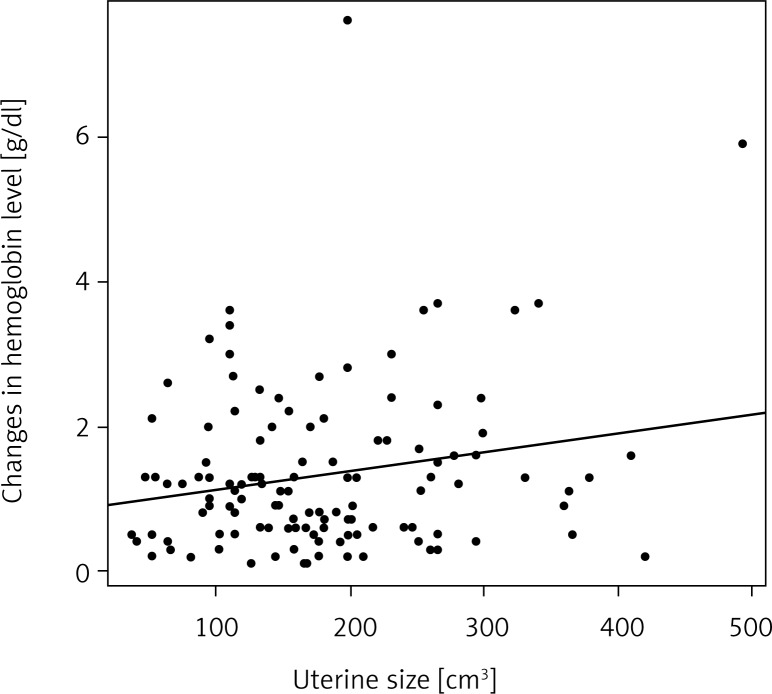
Results: There were no differences in patients' mean age. Parity was significantly higher in the VH group (VH 1.9 ± 0.7 vs. LAVH 1.5 ± 0.8; p = 0.008). No difference was found in the mean ± standard deviation (SD) uterine volume between vaginal hysterectomy and LAVH groups (179 ± 89 vs. 199 ± 88 cm(3)), respectively. The mean operative time was significantly longer for the LAVH group (83 ± 29 vs. 131 ± 30 min; p = 0.0001). The intraoperative blood loss (VH 1.3 ± 1.1 vs. LAVH 1.4 ± 0.9 g/dl; p = 0.2) and the rate of intra- and postoperative complications were similar in both groups studied. The mean discharge time was longer for LAVH than for VH (VH 4.2 ± 1.2 vs. LAVH 5.3 ± 1.3 days, p = 0.0001).
Conclusions: Laparoscopically assisted vaginal hysterectomy and VH are safe hysterectomy techniques for women with the myomatous uterus. Concerning the LAVH, the abdominal-pelvic exploration and the ability to perform adnexectomy safely represent the major advantages comparing with VH. Vaginal hysterectomy had a shorter operating time and the mild blood loss making it a suitable method of hysterectomy for cases in which the shortest duration of surgery and anesthesia is preferable.
Keywords: laparoscopically assisted vaginal hysterectomy (LAVH); uterine myomas; vaginal hysterectomy (VH).
Figures
References
-
- Su WH, Lee WL, Cheng MH, et al. Typical and atypical clinical presentation of uterine myomas. J Chin Med Assoc. 2012;75:487–493. - PubMed
-
- Wilcox LS, Koonin LM, Pokras R, et al. Hysterectomy in the United States 1988-1990. Obstet Gynecol. 1994;83:549–555. - PubMed
-
- Lepine LA, Hillis SD, Marchbanks PA, et al. Hysterectomy surveillance – United States, 1980-1993. MMWR CDC Surveill Summ. 1997;46:1–15. - PubMed
-
- Keshavarz H, Hillis SD, Kiele BA, et al. Hysterectomy surveillance – United States, 1994-1999. MMWR CDC Surveill Summ. 2002;51(SS-5):1–8.
-
- Wu JM, Wechter ME, Geller EJ, et al. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091–1095. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous