

Frailty and Short-Term Outcomes in Patients With Hip Fracture
- PMID: 26328238
- PMCID: PMC4536514
- DOI: 10.1177/2151458515591170
Frailty and Short-Term Outcomes in Patients With Hip Fracture
Abstract
Objectives: To assess the prevalence of frailty and its ability to predict short-term outcomes in older patients with hip fracture.
Design: Prospective cohort study.
Setting: University-affiliated community hospital.
Participants: Thirty-five patients aged ≥65 treated with hip fracture.
Measurements: Frailty was assessed using the 5 criteria of the Fried Frailty Index, modified for a post-fracture population. Cognitive impairment was assessed with the Montreal Cognitive Assessment (MoCA). The primary outcome was overall hospital complication rate. Secondary outcomes were length of stay (LOS) and specific complications. Differences between the frail and the non-frail were identified using chi-square analysis and analysis of variance (ANOVA) for categorical and continuous variables, respectively.
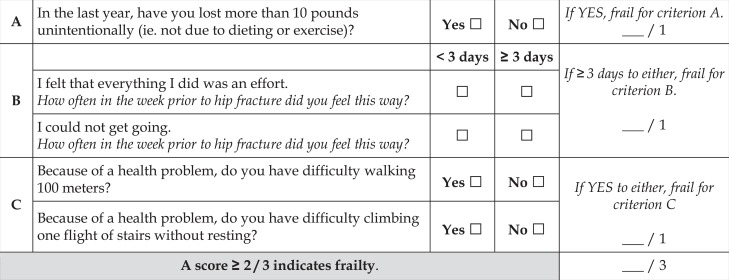
Results: Eighteen (51%) participants were frail. Seventeen (49%) had ≥1 hospital complication. Twelve (67%) frail patients versus 5 (29%) non-frail patients had a complication (P = .028). Mean LOS was longer in patients with frailty (7.3 ± 5.9 vs 4.1 ± 1.2 days, P = .038). Most were frail for the weakness criterion (94%), and few were frail for the physical activity criterion (9%). Excluding these criteria, we developed a 3-criteria frailty index (shrinking, exhaustion, and slowness) that identified an increased risk of complications (64.7% vs 33.3%, P = .061) and LOS (7.4 ± 6.1 vs 4.2 ± 1.3 days, P = .040) in participants with frailty. Among non-frail participants with a high MoCA score of ≥20 (n = 12), 2 (17%) had complications compared to 10 (71%) frail participants with a low MoCA score (n = 14).
Conclusion: Frailty is common in older patients with hip fracture and associated with increased LOS and postoperative complications. A low MoCA score, a hypothesized marker of more advanced cognitive frailty, may further increase risk. Frailty assessment has a role in prognostic discussion and care planning. The 3-criteria frailty index is an easily used tool with potential application in clinical practice.
Keywords: frailty; hip fracture; prognosis.
Conflict of interest statement
Figures
References
-
- National Center for Health Statistics. National Hospital Discharge Survey, 2010. Public-use data file and documentation. Web site http://www.cdc.gov/nchs/data/nhds/2average/2010ave2_dischargesage.pdf. Accessed June 6, 2015.
-
- Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc. 2003;51(3):364–370. - PubMed
-
- Leibson CL, Tosteson AN, Gabriel SE, Ransom JE, Melton LJ. Mortality, disability and nursing home use for persons with and without hip fracture: a population-based study. J Am Geriatr Soc. 2002;50(10):1644–1650. - PubMed
-
- Penrod JD, Litke A, Hawkes WG, et al. Heterogeneity in hip fracture patients: age, functional status, and comorbidity. J Am Geriatr Soc. 2007;55(3):407–413. - PubMed
-
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59(3):255–263. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
