

An unusual and challenging case of HIV-associated primary CNS Lymphoma with Hodgkin-like morphology and HIV encephalitis
- PMID: 26328586
- PMCID: PMC4557544
- DOI: 10.1186/s13000-015-0387-9
An unusual and challenging case of HIV-associated primary CNS Lymphoma with Hodgkin-like morphology and HIV encephalitis
Abstract
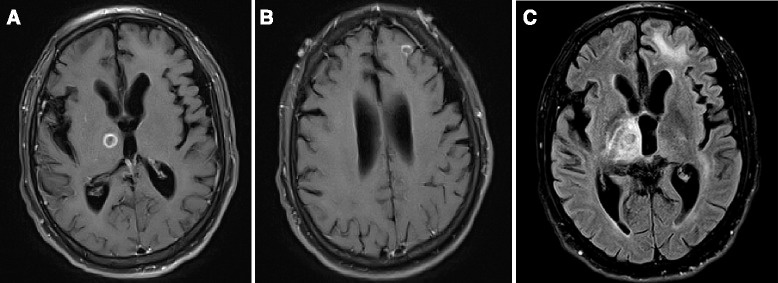
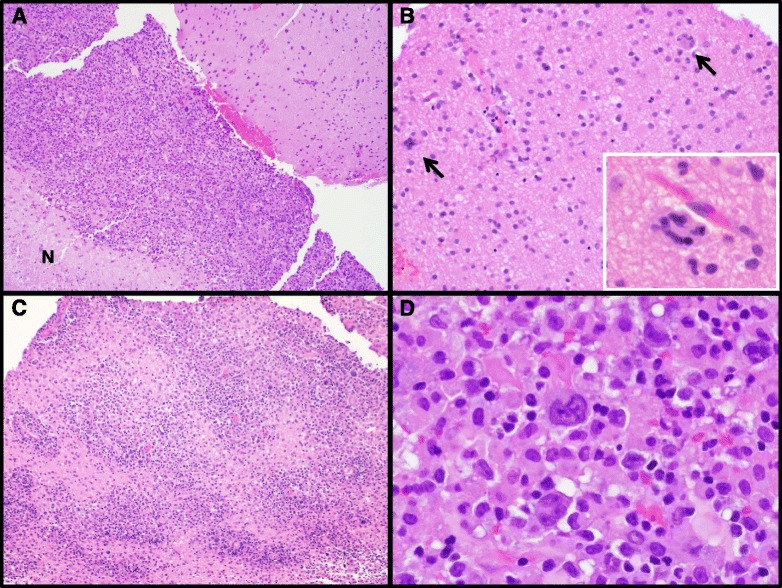
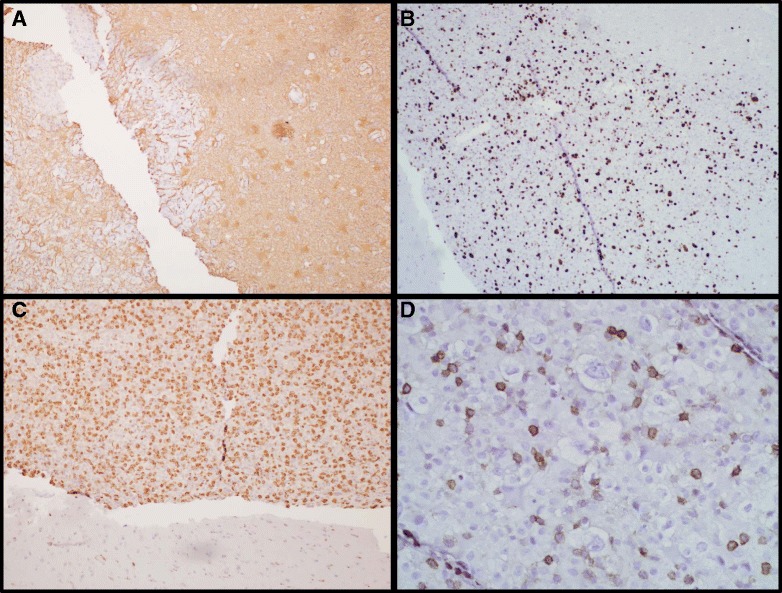
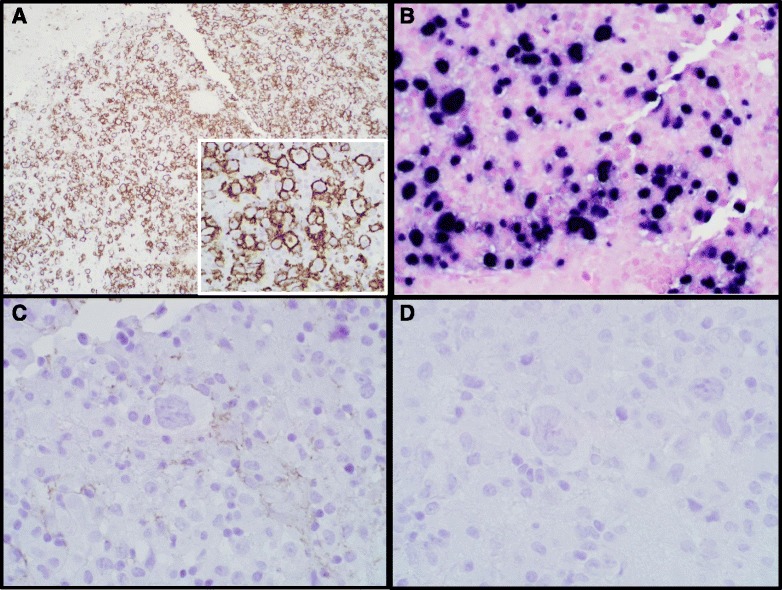
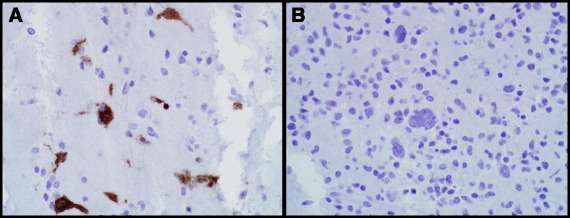
HIV-associated primary CNS lymphomas are well-recognized, almost exclusively EBV-driven neoplasms with poor clinical prognosis. We report a challenging, atypical case of an HIV-associated lymphoproliferative disorder with unusual morphologic features reminiscent of Hodgkin Lymphoma, accompanied by HIV encephalitis. A 52-year-old male presented with acute seizures after seven months of progressive neurocognitive decline that was clinically diagnosed as progressive supranuclear palsy. Clinical work-up revealed HIV infection along with two ring-enhancing lesions in the brain on MRI, and negative CSF EBV testing. Subsequent biopsy showed well-demarcated hypercellular regions in the brain comprised of scattered Reed-Sternberg-like cells in a background of small to medium-sized lymphocytes exhibiting focal angiocentricity and geographic necrosis. The atypical cells were positive for CD20, EBV, and CD79a, and negative for CD45, GFAP, CD15, CD30, and p24. These cells were admixed with numerous CD68-positive cells. The adjacent brain showed classic features of HIV encephalitis with perivascular, CD68 and p24-positive multinucleated giant cells. This case illustrates several diagnostic pitfalls in the work-up of HIV-associated brain lesions, as well as reporting a unique histomorphology for an HIV-related primary CNS lymphoproliferative disorder.
Figures
Similar articles
-
A malignant lymphoma with histological features and immunophenotypic profile intermediate between EBV-positive diffuse large B-cell lymphoma and EBV-positive classical Hodgkin lymphoma in a 67-year-old female: a "gray zone" lymphoma associated with Epstein-Barr virus in the elderly.Pathol Res Pract. 2012 Jun 15;208(6):363-7. doi: 10.1016/j.prp.2012.04.003. Epub 2012 May 7. Pathol Res Pract. 2012. PMID: 22572037
-
Composite recurrent hodgkin lymphoma and diffuse large B-cell lymphoma: one clone, two faces.Am J Clin Pathol. 2006 Aug;126(2):222-9. doi: 10.1309/DDGL-WRV3-KR91-64G7. Am J Clin Pathol. 2006. PMID: 16891197
-
Cytotoxic Epstein-Barr virus-positive large B cell lymphoma: a regulatory B cell-derived neoplasia?Histopathology. 2017 Mar;70(4):650-656. doi: 10.1111/his.13109. Epub 2016 Dec 20. Histopathology. 2017. PMID: 27782313
-
Epstein-Barr virus-positive diffuse large B-cell lymphomas of the elderly.Adv Anat Pathol. 2011 Sep;18(5):349-55. doi: 10.1097/PAP.0b013e318229bf08. Adv Anat Pathol. 2011. PMID: 21841405 Review.
-
Soft tissue non-Hodgkin lymphoma of shoulder in a HIV patient: a report of a case and review of the literature.World J Surg Oncol. 2008 Oct 21;6:111. doi: 10.1186/1477-7819-6-111. World J Surg Oncol. 2008. PMID: 18939988 Free PMC article. Review.
Cited by
-
Human Immunodeficiency Virus in the Brain-Culprit or Facilitator?Infect Dis (Auckl). 2018 Feb 14;11:1178633717752687. doi: 10.1177/1178633717752687. eCollection 2018. Infect Dis (Auckl). 2018. PMID: 29467577 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
