

Coverage-based treatment planning to accommodate delineation uncertainties in prostate cancer treatment
- PMID: 26328992
- PMCID: PMC4545100
- DOI: 10.1118/1.4928490
Coverage-based treatment planning to accommodate delineation uncertainties in prostate cancer treatment
Abstract
Purpose: To compare two coverage-based planning (CP) techniques with fixed margin-based (FM) planning for high-risk prostate cancer treatments, with the exclusive consideration of the dosimetric impact of delineation uncertainties of target structures and normal tissues.
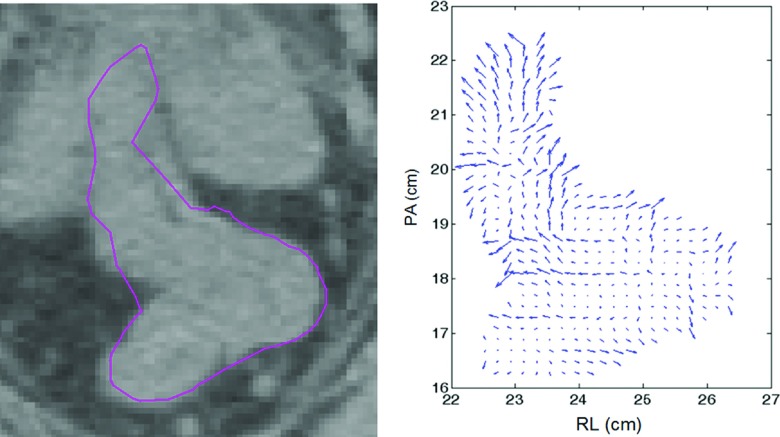
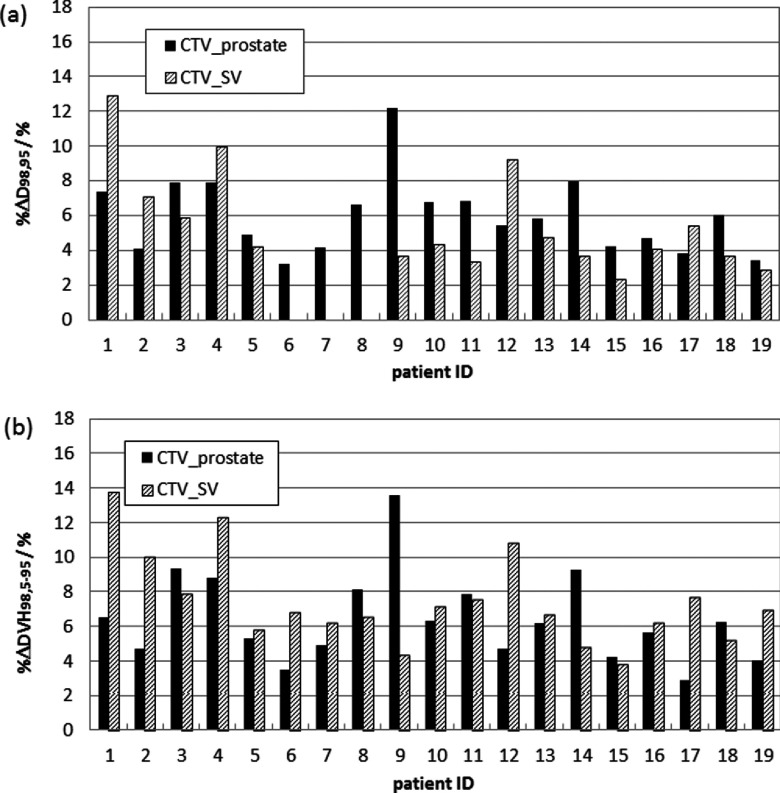
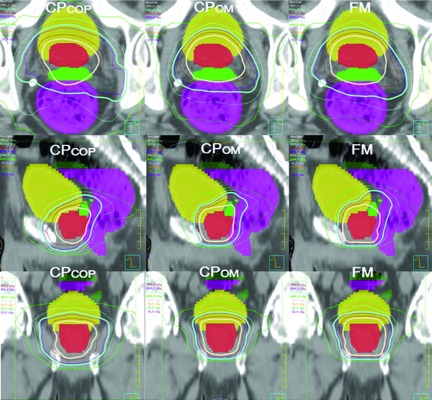
Methods: In this work, 19-patient data sets were involved. To estimate structure dose for each delineated contour under the influence of interobserver contour variability and CT image quality limitations, 1000 alternative structures were simulated by an average-surface-of-standard-deviation model, which utilized the patient-specific information of delineated structure and CT image contrast. An IMRT plan with zero planning-target-volume (PTV) margin on the delineated prostate and seminal vesicles [clinical-target-volume (CTV prostate) and CTVSV] was created and dose degradation due to contour variability was quantified by the dosimetric consequences of 1000 alternative structures. When D98 failed to achieve a 95% coverage probability objective D98,95 ≥ 78 Gy (CTV prostate) or D98,95 ≥ 66 Gy (CTVSV), replanning was performed using three planning techniques: (1) FM (PTV prostate margin = 4,5,6 mm and PTVSV margin = 4,5,7 mm for RL, PA, and SI directions, respectively), (2) CPOM which optimized uniform PTV margins for CTV prostate and CTVSV to meet the D98,95 objectives, and (3) CPCOP which directly optimized coverage-based objectives for all the structures. These plans were intercompared by computing percentile dose-volume histograms and tumor-control probability/normal tissue complication probability (TCP/NTCP) distributions.
Results: Inherent contour variability resulted in unacceptable CTV coverage for the zero-PTV-margin plans for all patients. For plans designed to accommodate contour variability, 18/19 CP plans were most favored by achieving desirable D98,95 and TCP/NTCP values. The average improvement of probability of complication free control was 9.3% for CPCOP plans and 3.4% for CPOM plans.
Conclusions: When the delineation uncertainties need to be considered for prostate patients, CP techniques can produce more desirable plans than FM plans for most patients. The relative advantages between CPCOP and CPOM techniques are patient specific.
Figures
References
-
- Huyskens D. P., Maingon P., Vanuytsel L., Remouchamps V., Roques T., Dubray B., Haas B., Kunz P., Coradi T., Bühlman R., Reddick R., Esch A. V., and Salamon E., “A qualitative and a quantitative analysis of an auto-segmentation module for prostate cancer,” Radiother. Oncol. 90, 337–345 (2009).10.1016/j.radonc.2008.08.007 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
