

Evaluation of lung cancer by enhanced dual-energy CT: association between three-dimensional iodine concentration and tumour differentiation
- PMID: 26329466
- PMCID: PMC4743448
- DOI: 10.1259/bjr.20150224
Evaluation of lung cancer by enhanced dual-energy CT: association between three-dimensional iodine concentration and tumour differentiation
Abstract
Objective: To investigate the correlation between iodine concentration of dual-energy CT (DECT) and histopathology of surgically resected primary lung cancers.
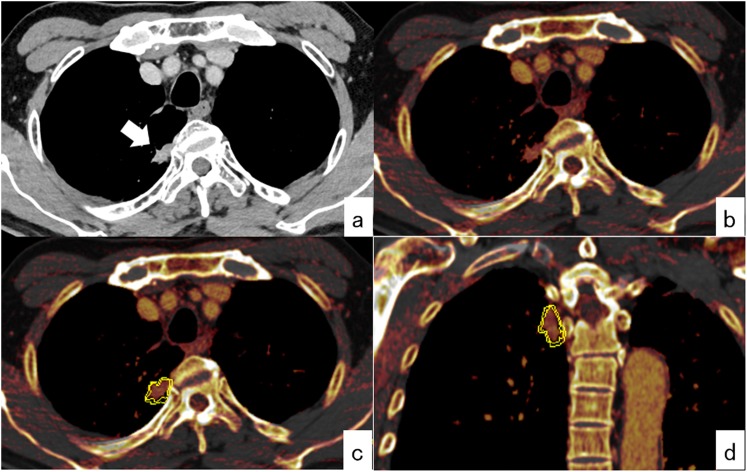
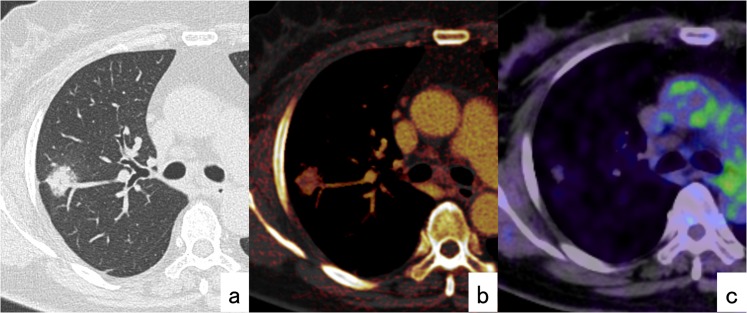
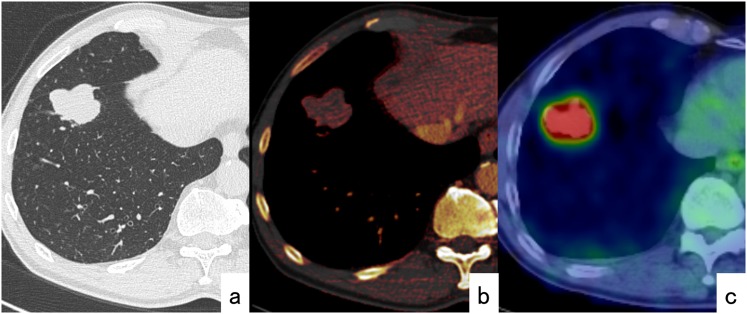
Methods: We reviewed the medical records, post-operative pathological records and pre-operative DECT images of patients who underwent surgical lung resection for primary lung cancer. After injection of iodinated contrast media, arterial and delayed phases were scanned using 140- and 80-kV tube voltages. Three-dimensional iodine concentration (iodine volume) of primary tumours was calculated using lung nodule application software.
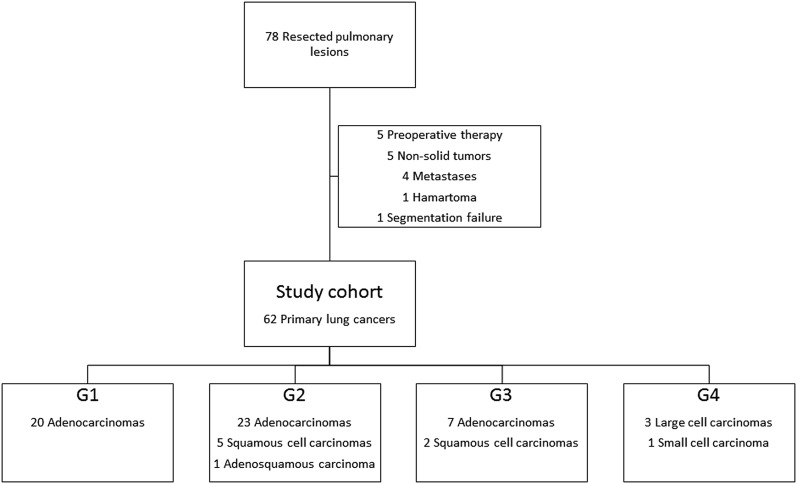
Results: A total of 60 patients (37 males and 23 females; age range, 39-84 years; mean age, 69 years) with 62 lung cancers were analysed. The resected tumours were histopathologically classified into well-differentiated (G1; n = 20), moderately differentiated (G2; n = 29), poorly differentiated (G3; n = 9) and undifferentiated (G4; n = 4) groups by degree of tumour differentiation (DTD). The mean ± standard deviation of iodine volume at the delayed phase was 59.6 ± 18.6 HU in G1 tumours, 46.5 ± 11.3 HU in G2 tumours, 34.3 ± 15.0 HU in G3 tumours and 28.8 ± 6.4 HU in G4 tumours; significant differences were observed between groups (p < 0.001). Univariate logistic regression analysis showed that iodine volumes both at the early and delayed phases were significantly correlated with DTD (p = 0.006 and p = 0.001, respectively), whereas gender, body weight and tumour size were not (p = 0.084, p = 0.062 and p = 0.391, respectively).
Conclusion: The iodine volume of lung cancers was significantly associated with their DTD. High-grade tumours tended to have lower iodine volumes than low-grade tumours.
Advances in knowledge: Iodine volume measured by DECT could be a valuable functional imaging method to estimate differentiation of primary lung cancer.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
