

Leukoencephalopathy resolution after atypical mycobacterial treatment: a case report
- PMID: 26329680
- PMCID: PMC4557863
- DOI: 10.1186/s12883-015-0415-0
Leukoencephalopathy resolution after atypical mycobacterial treatment: a case report
Abstract
Background: Association of leukoencephalopathy and atypical mycobacteriosis has been rarely reported. We present a case that is relevant for its unusual presentation and because it may shed further light on the pathogenic mechanisms underlying reversible encephalopathies.
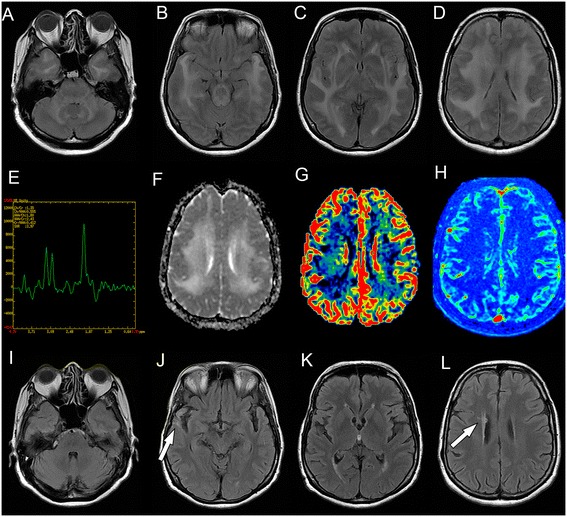
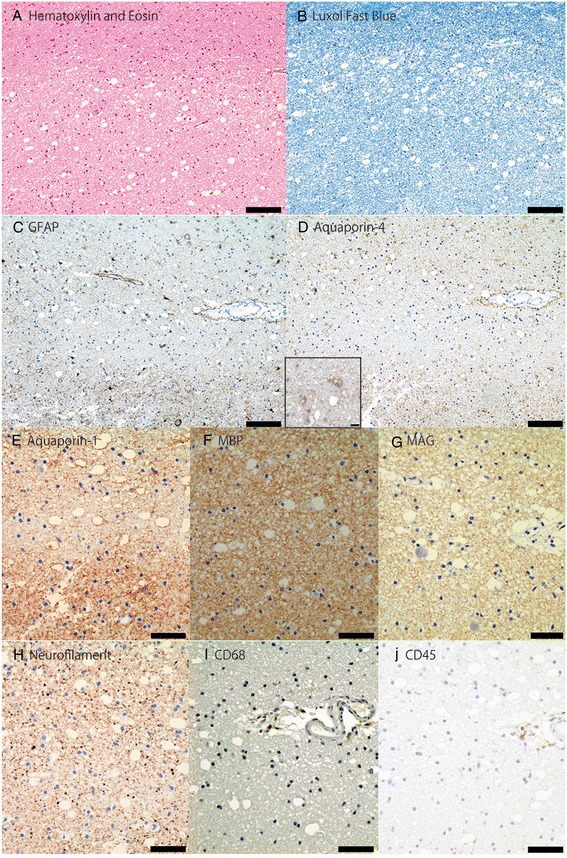
Case report: We report the case of a Hispanic 64-year-old woman with cognitive decline and extensive leukoencephalopathy. Magnetic resonance imaging revealed white-matter lesions with increased water diffusivity, without blood-brain-barrier disruption. Brain biopsy showed tissue rarefaction with vacuolation, mild inflammation, few reactive astrocytes and decreased aquaporin water-channel expression in the lesions. Six months later, she was diagnosed with atypical mycobacterial pulmonary infection. Brain lesions resolved after antimycobacterial treatment.
Conclusion: We hypothesize leukoencephalopathic changes and vasogenic edema were associated with decreased aquaporin expression. Further studies should clarify if reversible leukoencephalopathy has a causal relationship with decreased aquaporin expression and atypical mycobacterial infection, and mechanisms underlying leukoencephalopathy resolution after antimycobacterial treatment. This article may contribute to the understanding of pathogenic mechanisms underlying magnetic resonance imaging subcortical lesions and edema, which remain incompletely understood.
Figures
References
-
- Lee VH, Wijdicks EM, Manno EM, Rabinstein AA. Clinical spectrum of reversible posterior leukoencephalopathy syndrome. Arch Neurol. 2008;65:205–210. - PubMed
-
- Magaña SM, Matiello M, Pittock SJ, McKeon A, Lennon VA, Rabinstein AA, et al. Posterior reversible encephalopathy syndrome in neuromyelitis optica spectrum disorders. Neurology. 2009;72(8):712–717. doi: 10.1212/01.wnl.0000343001.36493.ae. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
