

Subarachnoid hemorrhage: who dies, and why?
- PMID: 26330064
- PMCID: PMC4556224
- DOI: 10.1186/s13054-015-1036-0
Subarachnoid hemorrhage: who dies, and why?
Abstract
Introduction: Subarachnoid hemorrhage (SAH) is a devastating form of stroke. Causes and mechanisms of in-hospital death after SAH in the modern era of neurocritical care remain incompletely understood.
Methods: We studied 1200 consecutive SAH patients prospectively enrolled in the Columbia University SAH Outcomes Project between July 1996 and January 2009. Analysis was performed to identify predictors of in-hospital mortality.
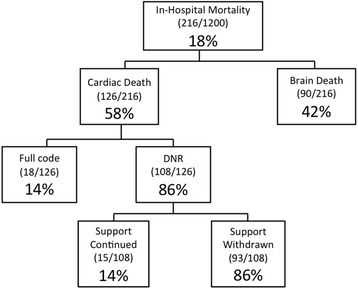
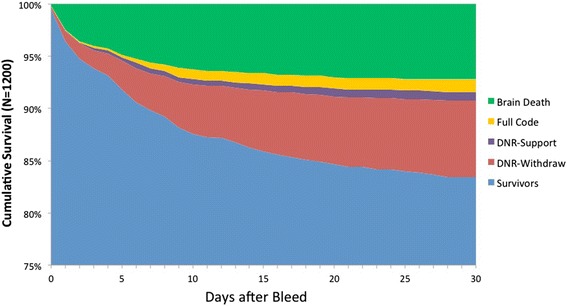
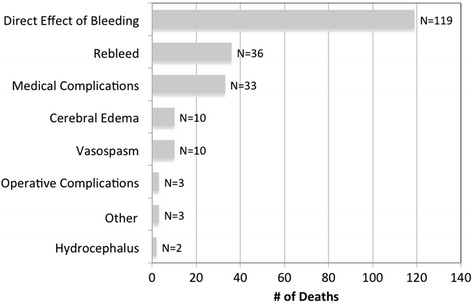
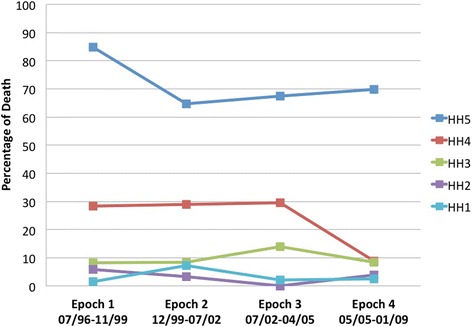
Results: In-hospital mortality was 18% (216/1200): 3% for Hunt-Hess grade 1 or 2, 9% for grade 3, 24% for grade 4, and 71% for grade 5. The most common adjudicated primary causes of death or neurological devastation leading to withdrawal of support were direct effects of the primary hemorrhage (55%), aneurysm rebleeding (17%), and medical complications (15%). Among those who died, brain death was declared in 42%, 50% were do-not-resuscitate at the time of cardiac death (86% of whom had life support actively withdrawn), and 8% died despite full support. Admission predictors of mortality were age, loss of consciousness at ictus, admission Glasgow Coma Scale score, large aneurysm size, Acute Physiology and Chronic Health Evaluation II (APACHE II) physiologic subscore, and Modified Fisher Scale score. Hospital complications that further increased the risk of dying in multivariable analysis included rebleeding, global cerebral edema, hypernatremia, clinical signs of brain stem herniation, hypotension of less than 90 mm Hg treated with pressors, pulmonary edema, myocardial ischemia, and hepatic failure. Delayed cerebral ischemia, defined as deterioration or infarction from vasospasm, did not predict mortality.
Conclusion: Strategies directed toward minimizing early brain injury and aneurysm rebleeding, along with prevention and treatment of medical complication, hold the best promise for further reducing mortality after SAH.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
