

Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR(CT): outcome and resource impacts study
- PMID: 26330417
- PMCID: PMC4677273
- DOI: 10.1093/eurheartj/ehv444
Clinical outcomes of fractional flow reserve by computed tomographic angiography-guided diagnostic strategies vs. usual care in patients with suspected coronary artery disease: the prospective longitudinal trial of FFR(CT): outcome and resource impacts study
Abstract
Aims: In symptomatic patients with suspected coronary artery disease (CAD), computed tomographic angiography (CTA) improves patient selection for invasive coronary angiography (ICA) compared with functional testing. The impact of measuring fractional flow reserve by CTA (FFRCT) is unknown.
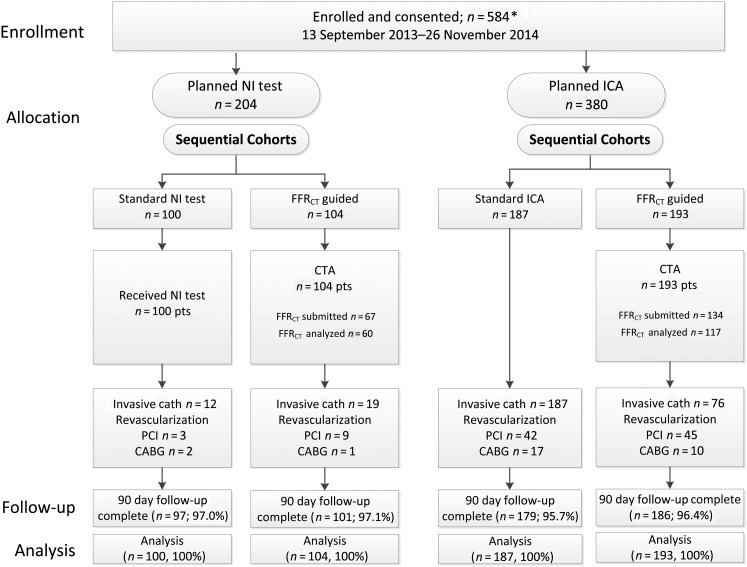
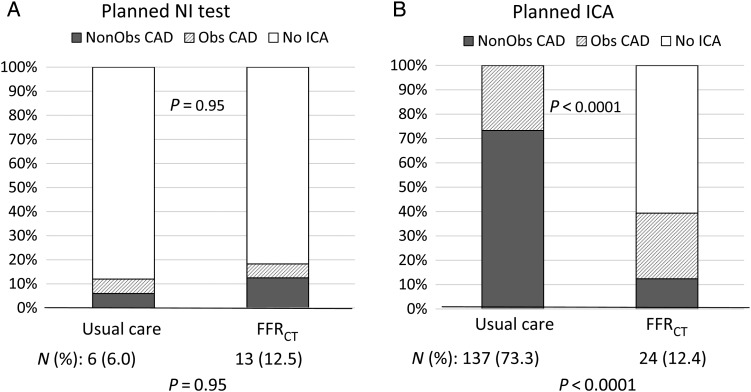
Methods and results: At 11 sites, 584 patients with new onset chest pain were prospectively assigned to receive either usual testing (n = 287) or CTA/FFR(CT) (n = 297). Test interpretation and care decisions were made by the clinical care team. The primary endpoint was the percentage of those with planned ICA in whom no significant obstructive CAD (no stenosis ≥50% by core laboratory quantitative analysis or invasive FFR < 0.80) was found at ICA within 90 days. Secondary endpoints including death, myocardial infarction, and unplanned revascularization were independently and blindly adjudicated. Subjects averaged 61 ± 11 years of age, 40% were female, and the mean pre-test probability of obstructive CAD was 49 ± 17%. Among those with intended ICA (FFR(CT)-guided = 193; usual care = 187), no obstructive CAD was found at ICA in 24 (12%) in the CTA/FFR(CT) arm and 137 (73%) in the usual care arm (risk difference 61%, 95% confidence interval 53-69, P< 0.0001), with similar mean cumulative radiation exposure (9.9 vs. 9.4 mSv, P = 0.20). Invasive coronary angiography was cancelled in 61% after receiving CTA/FFR(CT) results. Among those with intended non-invasive testing, the rates of finding no obstructive CAD at ICA were 13% (CTA/FFR(CT)) and 6% (usual care; P = 0.95). Clinical event rates within 90 days were low in usual care and CTA/FFR(CT) arms.
Conclusions: Computed tomographic angiography/fractional flow reserve by CTA was a feasible and safe alternative to ICA and was associated with a significantly lower rate of invasive angiography showing no obstructive CAD.
Keywords: Angina; Coronary computed tomographic angiography; Fractional flow reserve; Non-invasive testing.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Acute coronary syndromes: Utility of measuring fractional flow reserve by CT angiography in patients with suspected CAD.Nat Rev Cardiol. 2015 Nov;12(11):619. doi: 10.1038/nrcardio.2015.138. Epub 2015 Sep 15. Nat Rev Cardiol. 2015. PMID: 26370485 No abstract available.
-
FFR(CT): a new technology in search of a clinical application.Eur Heart J. 2015 Dec 14;36(47):3368-9. doi: 10.1093/eurheartj/ehv534. Epub 2015 Oct 7. Eur Heart J. 2015. PMID: 26450009 No abstract available.
References
-
- Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, Bugiardini R, Crea F, Cuisset T, Di Mario C, Ferreira JR, Gersh BJ, Gitt AK, Hulot JS, Marx N, Opie LH, Pfisterer M, Prescott E, Ruschitzka F, Sabaté M, Senior R, Taggart DP, van der Wall EE, Vrints CJ, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Knuuti J, Valgimigli M, Bueno H, Claeys MJ, Donner-Banzhoff N, Erol C, Frank H, Funck-Brentano C, Gaemperli O, Gonzalez-Juanatey JR, Hamilos M, Hasdai D, Husted S, James SK, Kervinen K, Kolh P, Kristensen SD, Lancellotti P, Maggioni AP, Piepoli MF, Pries AR, Romeo F, Rydén L, Simoons ML, Sirnes PA, Steg PG, Timmis A, Wijns W, Windecker S, Yildirir A, Zamorano JL. ESC Committee for Practice Guidelines; Document Reviewers. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34:2949–3003. - PubMed
-
- Douglas PS, Hoffmann U, Patel MR, Mark DB, Al-Khalidi HR, Cavanaugh B, Cole J, Dolor RJ, Fordyce CB, Huang M, Khan MA, Kosinski AS, Krucoff MW, Malhotra V, Picard MH, Udelson JE, Velazquez EJ, Yow E, Cooper LS, Lee KL; PROMISE Investigators. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med 2015;372:1291–1300. - PMC - PubMed
-
- Newby DE on behalf of the SCOT-HEART Investigators. CT coronary angiography in patients with suspected angina due to coronary heart disease (SCOT-HEART): an open-label, parallel-group, multicentre trial. Lancet 2015;385:2383–2391. - PubMed
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011;58:e44–e122. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
