

The Contribution of Cervicovaginal Infections to the Immunomodulatory Effects of Hormonal Contraception
- PMID: 26330510
- PMCID: PMC4556810
- DOI: 10.1128/mBio.00221-15
The Contribution of Cervicovaginal Infections to the Immunomodulatory Effects of Hormonal Contraception
Abstract
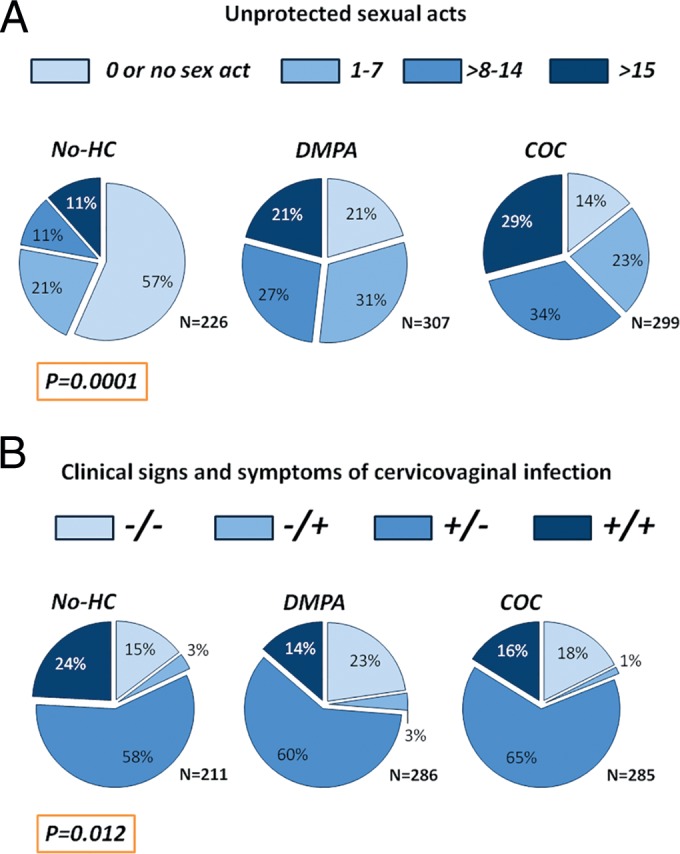
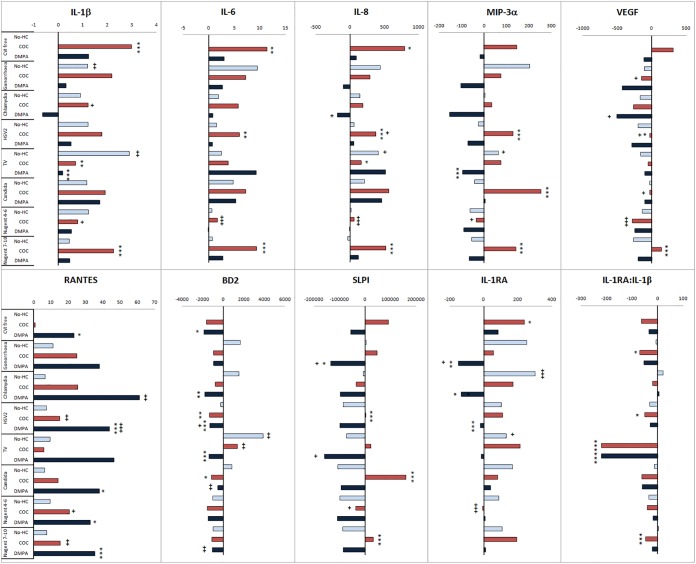
Particular types of hormonal contraceptives (HCs) and genital tract infections have been independently associated with risk of HIV-1 acquisition. We examined whether immunity in women using injectable depot medroxyprogesterone acetate (DMPA), combined oral contraceptives (COC), or no HCs differs by the presence of cervicovaginal infections. Immune mediators were quantified in cervical swabs from 832 HIV-uninfected reproductive-age Ugandans and Zimbabweans. Bacterial infections and HIV were diagnosed by PCR, genital herpes serostatus by enzyme-linked immunosorbent assay (ELISA), altered microflora by Nugent score, and Trichomonas vaginalis and Candida albicans infection by wet mount. Generalized linear models utilizing Box-Cox-Power transformation examined associations between levels of mediators, infection status, and HCs. In no-HC users, T. vaginalis was associated with broadest spectrum of aberrant immunity (higher interleukin 1β [IL-1β], IL-8, macrophage inflammatory protein 3α [MIP-3α], β-defensin 2 [BD2], and IL-1 receptor antigen [IL-1RA]). In women with a normal Nugent score and no genital infection, compared to the no-HC group, COC users showed higher levels of IL-1β, IL-6, IL-8, and IL-1RA, while DMPA users showed higher levels of RANTES and lower levels of BD2, both associated with HIV seroconversion. These effects of COC were blunted in the presence of gonorrhea, chlamydia, trichomoniasis, candidiasis, and an abnormal Nugent score; however, RANTES was increased among COC users with herpes, chlamydia, and abnormal Nugent scores. The effect of DMPA was exacerbated by lower levels of IL-1RA in gonorrhea, chlamydia, or herpes, SLPI in gonorrhea, and IL-1β, MIP-3α, and IL-1RA/IL1β ratio in trichomoniasis. Thus, the effects of HC on cervical immunity depend on the genital tract microenvironment, and a weakened mucosal barrier against HIV may be a combined resultant of genital tract infections and HC use.
Importance: In this article, we show that in young reproductive-age women most vulnerable to HIV, hormonal contraceptives are associated with altered cervical immunity in a manner dependent on the presence of genital tract infections. Through altered immunity, hormones may predispose women to bacterial and viral pathogens; conversely, a preexisting specific infection or disturbed vaginal microbiota may suppress the immune activation by levonorgestrel or exacerbate the suppressed immunity by DMPA, thus increasing HIV risk by their cumulative action. Clinical studies assessing the effects of contraception on HIV susceptibility and mucosal immunity may generate disparate results in populations that differ by microbiota background or prevalence of undiagnosed genital tract infections. A high prevalence of asymptomatic infections among HC users that remain undiagnosed and untreated raises even more concerns in light of their combined effects on biomarkers of HIV risk. The molecular mechanisms of the vaginal microbiome's simultaneous interactions with hormones and HIV remain to be elucidated.
Copyright © 2015 Fichorova et al.
Figures
Similar articles
-
A Longitudinal Assessment of Cervical Inflammation and Immunity Associated with HIV-1 Infection, Hormonal Contraception, and Pregnancy.AIDS Res Hum Retroviruses. 2018 Oct;34(10):889-899. doi: 10.1089/AID.2018.0022. Epub 2018 Sep 5. AIDS Res Hum Retroviruses. 2018. PMID: 30047279 Free PMC article.
-
Cervical inflammation and immunity associated with hormonal contraception, pregnancy, and HIV-1 seroconversion.J Acquir Immune Defic Syndr. 2014 Jun 1;66(2):109-17. doi: 10.1097/QAI.0000000000000103. J Acquir Immune Defic Syndr. 2014. PMID: 24413042
-
Aberrant cervical innate immunity predicts onset of dysbiosis and sexually transmitted infections in women of reproductive age.PLoS One. 2020 Jan 8;15(1):e0224359. doi: 10.1371/journal.pone.0224359. eCollection 2020. PLoS One. 2020. PMID: 31914129 Free PMC article.
-
Hormonal contraception decreases bacterial vaginosis but oral contraception may increase candidiasis: implications for HIV transmission.AIDS. 2013 Aug 24;27(13):2141-53. doi: 10.1097/QAD.0b013e32836290b6. AIDS. 2013. PMID: 23660575
-
Hormonal Contraceptives and the Acquisition of Sexually Transmitted Infections: An Updated Systematic Review.Sex Transm Dis. 2019 May;46(5):290-296. doi: 10.1097/OLQ.0000000000000975. Sex Transm Dis. 2019. PMID: 30628946
Cited by
-
Cervical and systemic innate immunity predictors of HIV risk linked to genital herpes acquisition and time from HSV-2 seroconversion.Sex Transm Infect. 2023 Aug;99(5):311-316. doi: 10.1136/sextrans-2022-055458. Epub 2022 Sep 14. Sex Transm Infect. 2023. PMID: 36104248 Free PMC article.
-
Mechanisms of sexually transmitted infection-induced inflammation in women: implications for HIV risk.J Int AIDS Soc. 2019 Aug;22 Suppl 6(Suppl Suppl 6):e25346. doi: 10.1002/jia2.25346. J Int AIDS Soc. 2019. PMID: 31468677 Free PMC article.
-
The relationship between sex hormones, the vaginal microbiome and immunity in HIV-1 susceptibility in women.Dis Model Mech. 2018 Aug 28;11(9):dmm035147. doi: 10.1242/dmm.035147. Dis Model Mech. 2018. PMID: 30154116 Free PMC article. Review.
-
Injectable Contraceptives Differentially Affect Select CD4+ HIV-1 Target Cells in the Genital Tract but Not Systemically: Implications for HIV-1 Acquisition.Am J Reprod Immunol. 2025 May;93(5):e70093. doi: 10.1111/aji.70093. Am J Reprod Immunol. 2025. PMID: 40349359 Free PMC article. Clinical Trial.
-
Biomarkers of Cervical Inflammation and Immunity Associated with Cervical Shedding of HIV-1.AIDS Res Hum Retroviruses. 2016 May;32(5):443-51. doi: 10.1089/AID.2015.0088. Epub 2016 Jan 26. AIDS Res Hum Retroviruses. 2016. PMID: 26650885 Free PMC article.
References
-
- Mugo NR, Heffron R, Donnell D, Wald A, Were EO, Rees H, Celum C, Kiarie JN, Cohen CR, Kayintekore K, Baeten JM, Partners in Prevention HSV/HIV Transmission Study Team . 2011. Increased risk of HIV-1 transmission in pregnancy: a prospective study among African HIV-1-serodiscordant couples. AIDS 25:1887–1895. doi:10.1097/QAD.0b013e32834a9338. - DOI - PMC - PubMed
-
- Gray RH, Li X, Kigozi G, Serwadda D, Brahmbhatt H, Wabwire-Mangen F, Nalugoda F, Kiddugavu M, Sewankambo N, Quinn TC, Reynolds SJ, Wawer MJ. 2005. Increased risk of incident HIV during pregnancy in Rakai, Uganda: a prospective study. Lancet 366:1182–1188. doi:10.1016/S0140-6736(05)67481-8. - DOI - PubMed
-
- Heffron R, Donnell D, Rees H, Celum C, Mugo N, Were E, de Bruyn G, Nakku-Joloba E, Ngure K, Kiarie J, Coombs RW, Baeten JM, Partners in Prevention HSV/HIV Transmission Study Team . 2012. Use of hormonal contraceptives and risk of HIV-1 transmission: a prospective cohort study. Lancet Infect Dis 12:19–26. doi:10.1016/S1473-3099(11)70247-X. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
