

Dual antiplatelet therapy in stroke and ICAS: Subgroup analysis of CHANCE
- PMID: 26330567
- PMCID: PMC4603889
- DOI: 10.1212/WNL.0000000000001972
Dual antiplatelet therapy in stroke and ICAS: Subgroup analysis of CHANCE
Abstract
AB OBJECTIVE: We aimed to investigate whether the efficacy and safety of clopidogrel plus aspirin vs aspirin alone were consistent between patients with and without intracranial arterial stenosis (ICAS), in the Clopidogrel in High-Risk Patients with Acute Non-disabling Cerebrovascular Events (CHANCE) trial.
Methods: We assessed the interaction of the treatment effects of the 2 antiplatelet therapies among patients with and without ICAS, identified by magnetic resonance angiography (MRA) in CHANCE (ClinicalTrials.gov identifier NCT00979589).
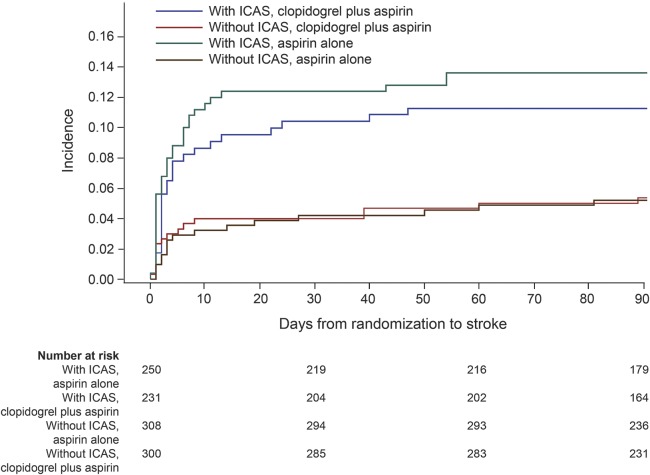
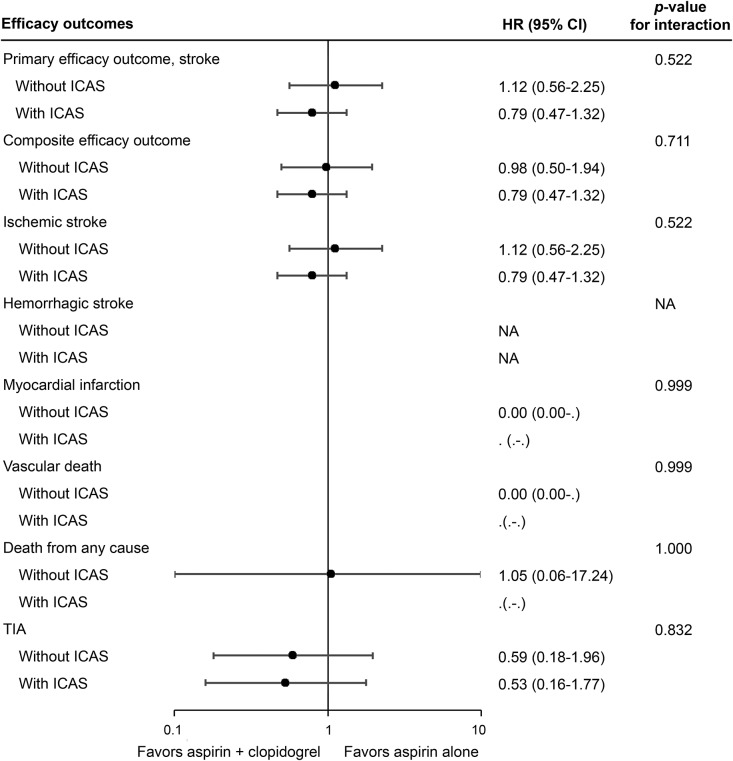
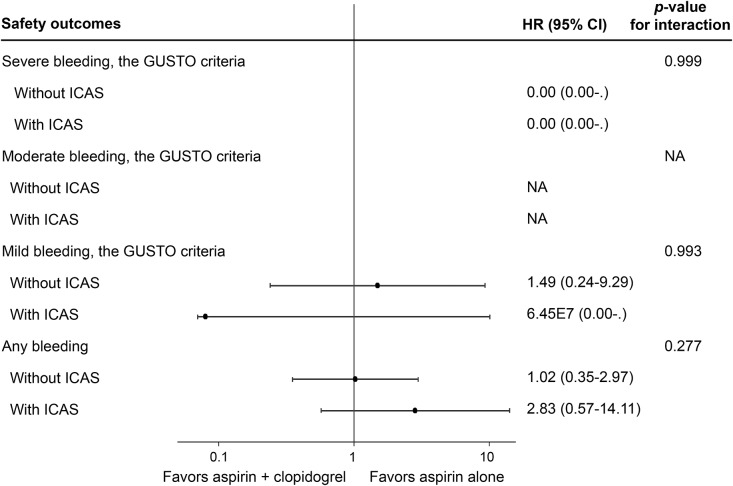
Results: Overall, 1,089 patients with MRA images available in CHANCE were included in this subanalysis, 608 patients (55.8%) with ICAS and 481 (44.2%) without. Patients with ICAS had higher rates of recurrent stroke (12.5% vs 5.4%; p<0.0001) at 90 days than those without. But there was no statistically significant treatment by presence of ICAS interaction on either the primary outcome of any stroke (hazard ratio for clopidogrel plus aspirin vs aspirin alone: 0.79 [0.47-1.32] vs 1.12 [0.56-2.25]; interaction p=0.522) or the safety outcome of any bleeding event (interaction p=0.277).
Conclusions: The results indicated higher rate of recurrent stroke in minor stroke or high-risk TIA patients with ICAS than in those without. However, there was no significant difference in the response to the 2 antiplatelet therapies between patients with and without ICAS in the CHANCE trial. Classification of evidence: This study provides Class II evidence that for patients with acute minor stroke or TIA with and without ICAS identified by MRA, clopidogrel plus aspirin is not significantly different than aspirin alone in preventing recurrent stroke.
© 2015 American Academy of Neurology.
Figures
References
-
- Markus HS, Droste DW, Kaps M, et al. Dual antiplatelet therapy with clopidogrel and aspirin in symptomatic carotid stenosis evaluated using Doppler embolic signal detection: the Clopidogrel and Aspirin for Reduction of Emboli in Symptomatic Carotid Stenosis (CARESS) Trial. Circulation 2005;111:2233–2240. - PubMed
-
- Wong KS, Chen C, Fu J, et al. Clopidogrel Plus Aspirin Versus Aspirin Alone for Reducing Embolisation in Patients with Acute Symptomatic Cerebral or Carotid Artery Stenosis (CLAIR Study): a randomised, open-label, blinded-endpoint trial. Lancet Neurol 2010;9:489–497. - PubMed
-
- Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11–19. - PubMed
-
- Feske SK. A little good. Circulation 2013;128:1598–1599. - PubMed
-
- Hankey GJ. Dual antiplatelet therapy in acute transient ischemic attack and minor stroke. N Engl J Med 2013;369:82–83. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical