

Stent mal-apposition with resorption of intramural hematoma with spontaneous coronary artery dissection
- PMID: 26331116
- PMCID: PMC4536472
- DOI: 10.3978/j.issn.2223-3652.2015.04.05
Stent mal-apposition with resorption of intramural hematoma with spontaneous coronary artery dissection
Abstract
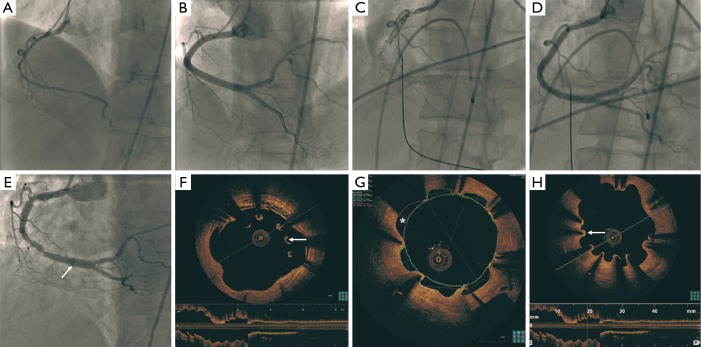
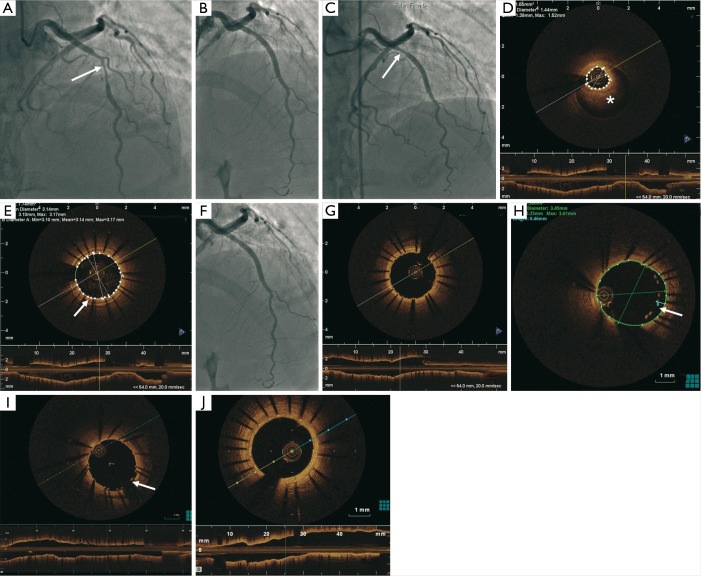
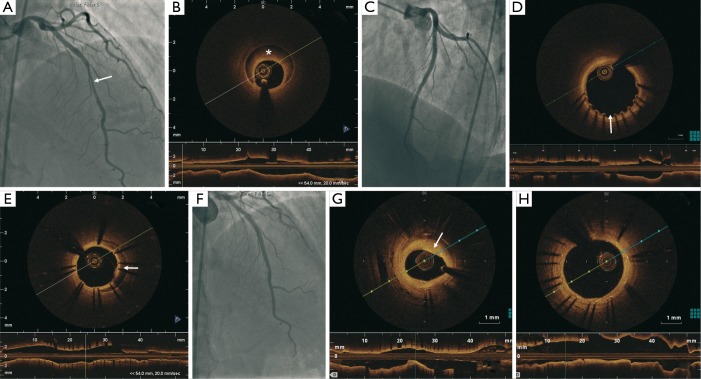
Spontaneous coronary artery dissection (SCAD) is an infrequent cause of acute coronary syndrome (ACS). Conservative management is typically recommended but revascularization may be necessary if ongoing ischemia or adverse anatomical characteristics are present. Percutaneous coronary intervention (PCI) of SCAD can be fraught with challenges, and intracoronary imaging with optical coherence tomography (OCT) may provide insights on optimizing the acute results and identify long-term stent-related adverse events. We report three cases of SCAD treated with drug-eluting stents (DES) with OCT follow-up showing stent mal-apposition at different stages of follow-up. The clinical significance of these OCT findings and management options are discussed.
Keywords: Angiography; arterial occlusive disease; coronary artery disease; optical coherence tomography (OCT); percutaneous coronary intervention (PCI).
Conflict of interest statement
Figures


References
-
- Lempereur M, Fung A, Saw J. OCT showing large arcs of malapposition, areas of evagination, and multiple areas of uncovered stent struts. Asvide 2015;2:072. Available online: http://www.asvide.com/articles/619
-
- Lempereur M, Fung A, Saw J. OCT demonstrating IMH proximal to the stent and tacked-up IMH in the wall of the stented segment. Asvide 2015;2:073. Available online: http://www.asvide.com/articles/620
-
- Lempereur M, Fung A, Saw J. OCT 15 days later showed patent stents but mild malapposition at the proximal edge of the proximal stent (250 µm) and persistent IMH covered by the stents. Asvide 2015;2:074. Available online: http://www.asvide.com/articles/621
-
- Saw J, Sedlak T, Ganesh SK, et al. Cardiology patient page. Spontaneous coronary artery dissection (SCAD). Circulation 2015;131:e3-5. - PubMed
-
- Saw J. Spontaneous coronary artery dissection. Can J Cardiol 2013;29:1027-33. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous