

Ovarian carcinoma patient derived xenografts reproduce their tumor of origin and preserve an oligoclonal structure
- PMID: 26334103
- PMCID: PMC4695063
- DOI: 10.18632/oncotarget.5069
Ovarian carcinoma patient derived xenografts reproduce their tumor of origin and preserve an oligoclonal structure
Abstract
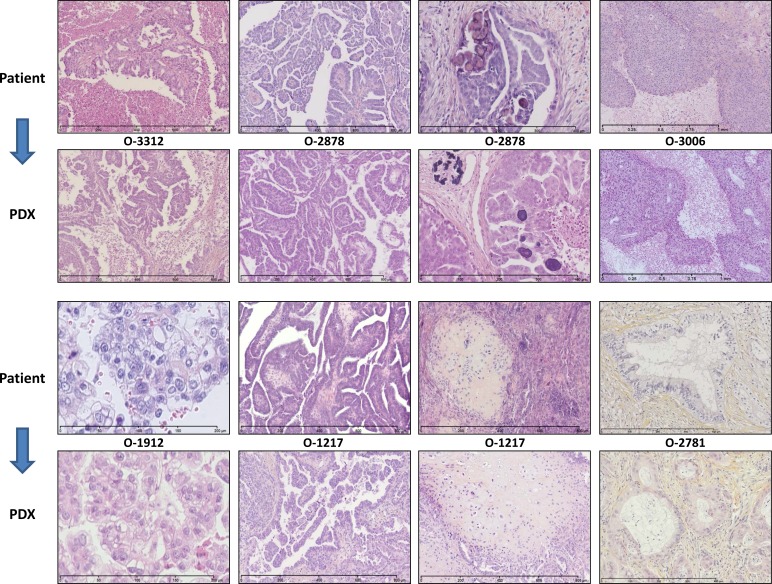
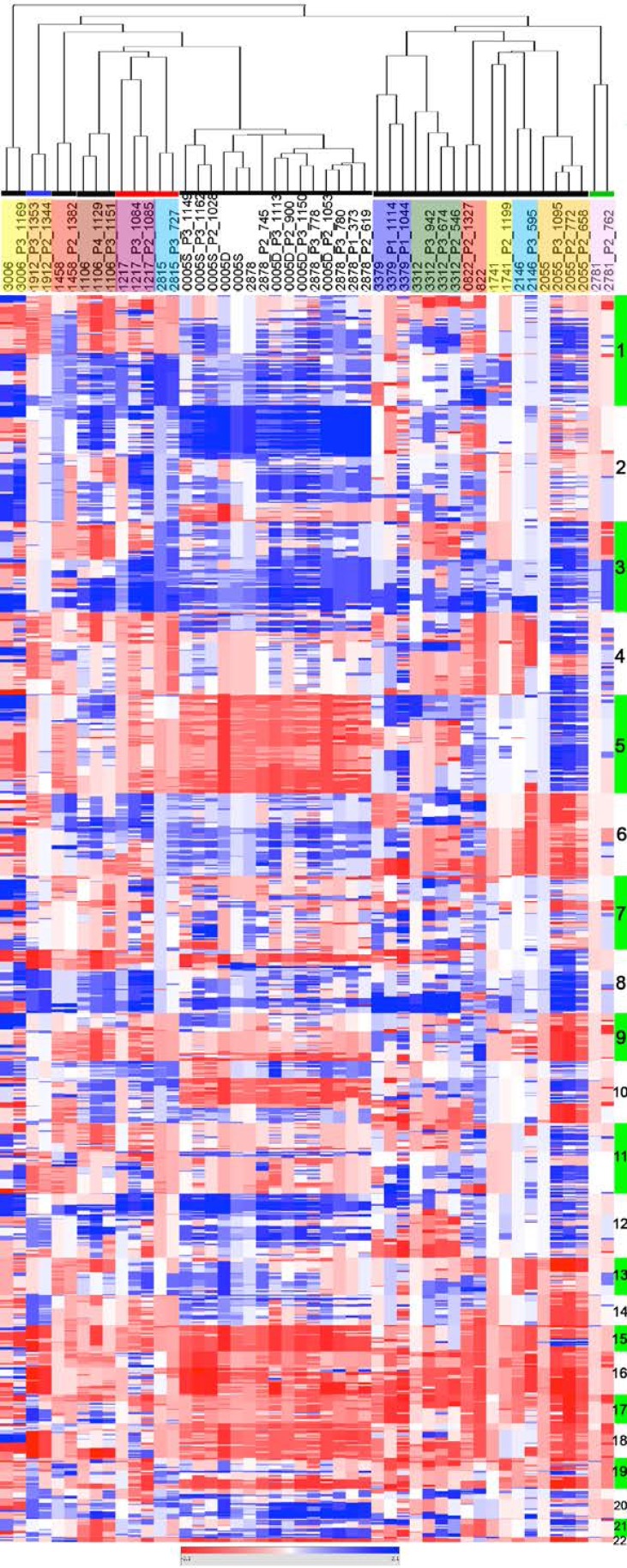
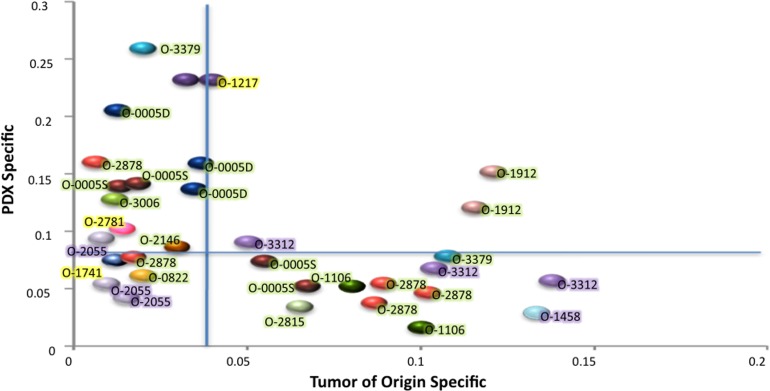
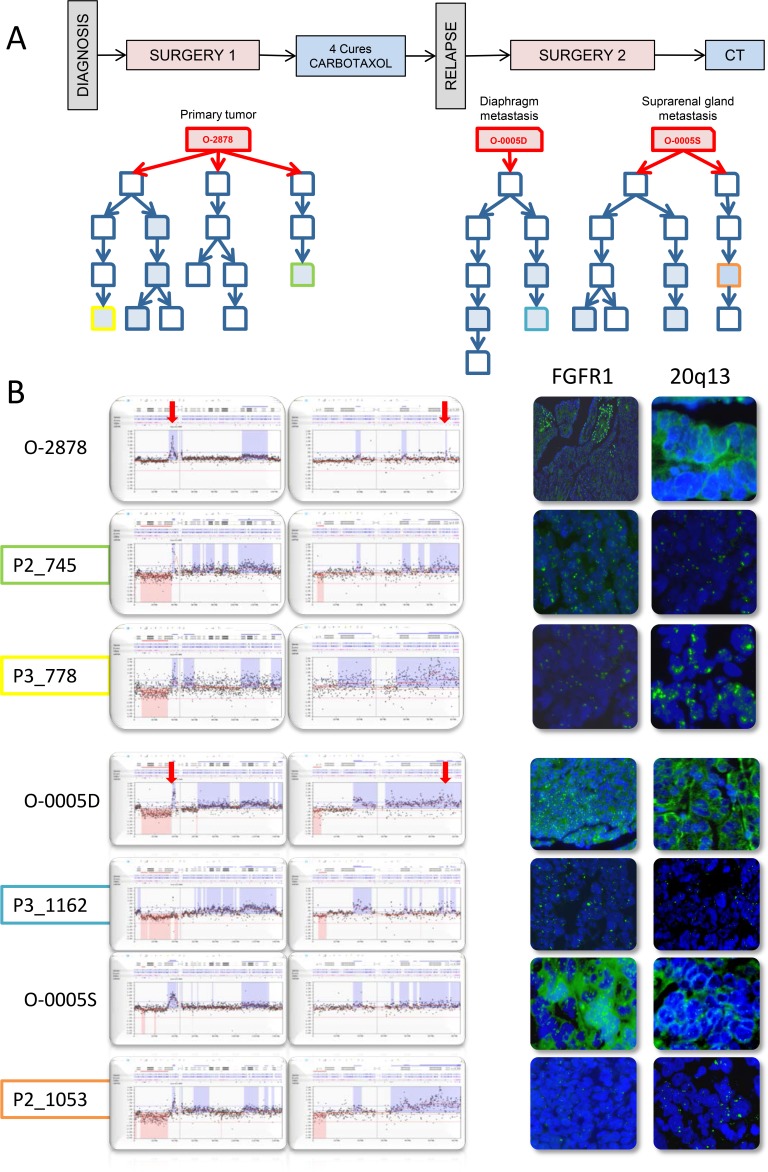
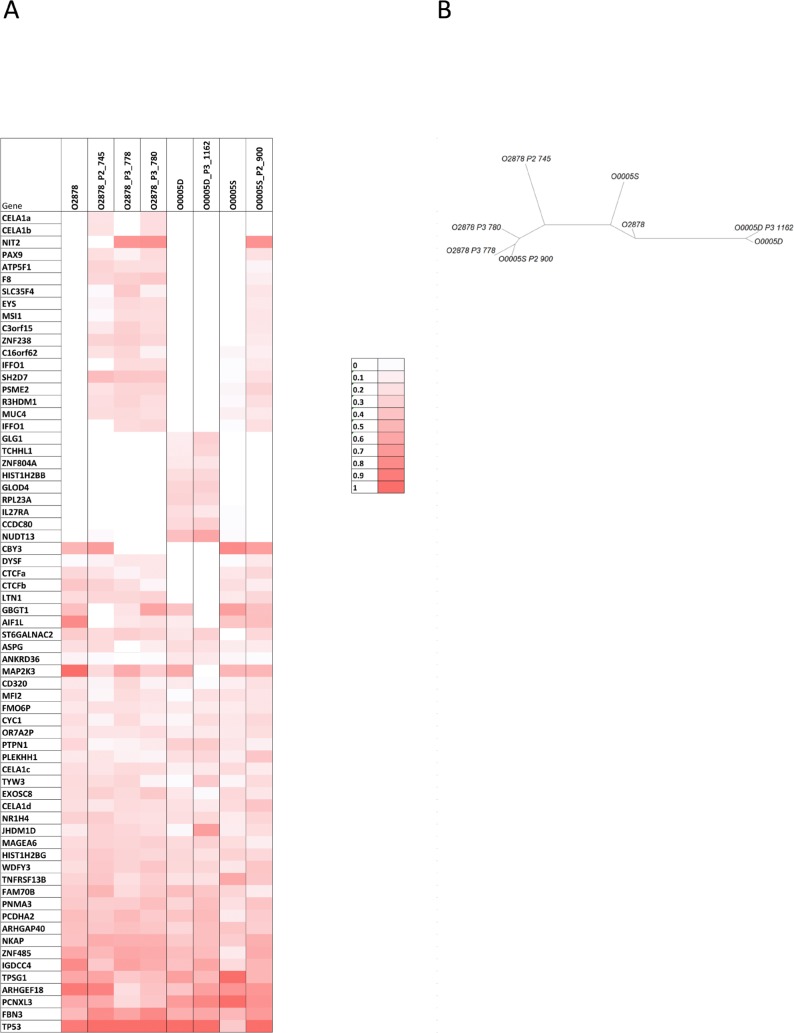
Advanced Epithelial Ovarian Cancer (EOC) patients frequently relapse by 24 months and develop resistant disease. Research on EOC therapies relies on cancer cell lines established decades ago making Patient Derived Xenografts (PDX) attractive models, because they are faithful representations of the original tumor. We established 35 ovarian cancer PDXs resulting from the original graft of 77 EOC samples onto immuno-compromised mice. PDXs covered the diversity of EOC histotypes and graft take was correlated with early patient death. Fourteen PDXs were characterized at the genetic and histological levels. PDXs reproduced phenotypic features of the ovarian tumors of origin and conserved the principal characteristics of the original copy number change (CNC) profiles over several passages. However, CNC fluctuations in specific subregions comparing the original tumor and the PDXs indicated the oligoclonal nature of the original tumors. Detailed analysis by CGH, FISH and exome sequencing of one case, for which several tumor nodules were sampled and grafted, revealed that PDXs globally maintained an oligoclonal structure. No overgrowth of a particular subclone present in the original tumor was observed in the PDXs. This suggested that xenotransplantation of ovarian tumors and growth as PDX preserved at least in part the clonal diversity of the original tumor. We believe our data reinforce the potential of PDX as exquisite tools in pre-clinical assays.
Keywords: CNC; PDX; mutations; oligoclonality; ovarian cancer.
Conflict of interest statement
No conflict of interest was reported by the authors.
Figures
Similar articles
-
Genome-wide methylation profiling of ovarian cancer patient-derived xenografts treated with the demethylating agent decitabine identifies novel epigenetically regulated genes and pathways.Genome Med. 2016 Oct 20;8(1):107. doi: 10.1186/s13073-016-0361-5. Genome Med. 2016. PMID: 27765068 Free PMC article.
-
Breast tumor PDXs are genetically plastic and correspond to a subset of aggressive cancers prone to relapse.Mol Oncol. 2014 Mar;8(2):431-43. doi: 10.1016/j.molonc.2013.11.010. Epub 2013 Dec 19. Mol Oncol. 2014. PMID: 24394560 Free PMC article. Clinical Trial.
-
Patient-Derived Xenograft Models of Epithelial Ovarian Cancer for Preclinical Studies.Cancer Res Treat. 2017 Oct;49(4):915-926. doi: 10.4143/crt.2016.322. Epub 2017 Jan 4. Cancer Res Treat. 2017. PMID: 28052650 Free PMC article.
-
Ovarian and cervical cancer patient derived xenografts: The past, present, and future.Gynecol Oncol. 2015 Aug;138(2):486-91. doi: 10.1016/j.ygyno.2015.05.022. Epub 2015 May 27. Gynecol Oncol. 2015. PMID: 26026736 Review.
-
Patient Derived Xenografts for Genome-Driven Therapy of Osteosarcoma.Cells. 2021 Feb 17;10(2):416. doi: 10.3390/cells10020416. Cells. 2021. PMID: 33671173 Free PMC article. Review.
Cited by
-
Humanized Patient-derived Xenograft Models of Disseminated Ovarian Cancer Recapitulate Key Aspects of the Tumor Immune Environment within the Peritoneal Cavity.Cancer Res Commun. 2023 Feb 22;3(2):309-324. doi: 10.1158/2767-9764.CRC-22-0300. eCollection 2023 Feb. Cancer Res Commun. 2023. PMID: 36860657 Free PMC article.
-
Genome-wide methylation profiling of ovarian cancer patient-derived xenografts treated with the demethylating agent decitabine identifies novel epigenetically regulated genes and pathways.Genome Med. 2016 Oct 20;8(1):107. doi: 10.1186/s13073-016-0361-5. Genome Med. 2016. PMID: 27765068 Free PMC article.
-
Establishment of the PDTX model of gynecological tumors.Am J Transl Res. 2019 Jun 15;11(6):3779-3789. eCollection 2019. Am J Transl Res. 2019. PMID: 31312388 Free PMC article.
-
Three-Dimensional Modelling of Ovarian Cancer: From Cell Lines to Organoids for Discovery and Personalized Medicine.Front Bioeng Biotechnol. 2022 Feb 10;10:836984. doi: 10.3389/fbioe.2022.836984. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 35223797 Free PMC article. Review.
-
Challenges in Stratifying the Molecular Variability of Patient-Derived Colon Tumor Xenografts.Biomed Res Int. 2018 Dec 19;2018:2954208. doi: 10.1155/2018/2954208. eCollection 2018. Biomed Res Int. 2018. PMID: 30662905 Free PMC article.
References
-
- Cannistra SA. Cancer of the ovary. N Engl J Med. 2004;351:2519–2529. - PubMed
-
- Colombo N, Peiretti M, Parma G, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21 Suppl 5:v23–30. - PubMed
-
- Colombo PE, Fabbro M, Theillet C, et al. Sensitivity and resistance to treatment in the primary management of epithelial ovarian cancer. Crit Rev Oncol Hematol. 2014;89:207–216. - PubMed
-
- Colombo PE, Mourregot A, Fabbro M, et al. Aggressive surgical strategies in advanced ovarian cancer: a monocentric study of 203 stage IIIC and IV patients. Eur J Surg Oncol. 2009;35:135–143. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
