

Treatment Outcomes in Stage I Lung Cancer: A Comparison of Surgery and Stereotactic Body Radiation Therapy
- PMID: 26334753
- PMCID: PMC4695298
- DOI: 10.1097/JTO.0000000000000680
Treatment Outcomes in Stage I Lung Cancer: A Comparison of Surgery and Stereotactic Body Radiation Therapy
Abstract
Introduction: The relative roles of surgery and stereotactic body radiation therapy in stage I non-small-cell lung cancer (NSCLC) are evolving particularly for marginally operable patients. Because there is limited prospective comparative data for these treatment modalities, we evaluated their relative use and outcomes at the population level using a national database.
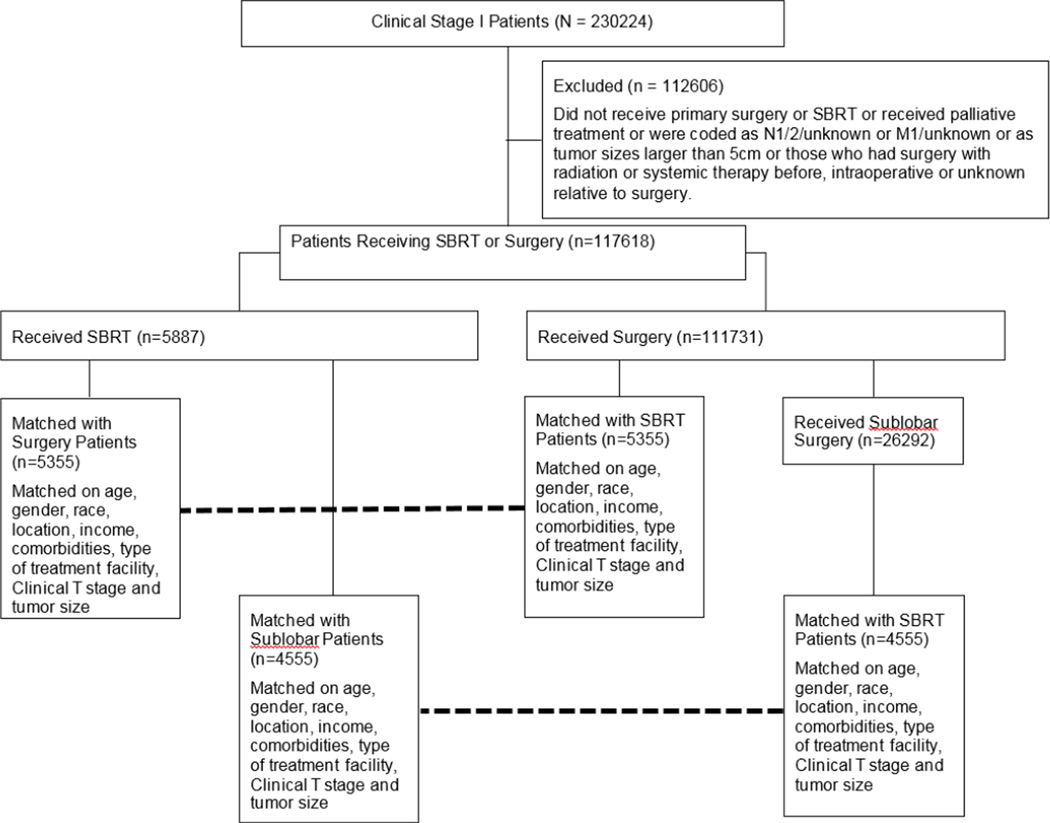
Methods: Patient variables and treatment-related outcomes were abstracted for patients with clinical stage I NSCLC from the National Cancer Database. Patients receiving surgery were compared with those undergoing stereotactic body radiation therapy (SBRT) in exploratory unmatched and subsequent propensity matched analyses.
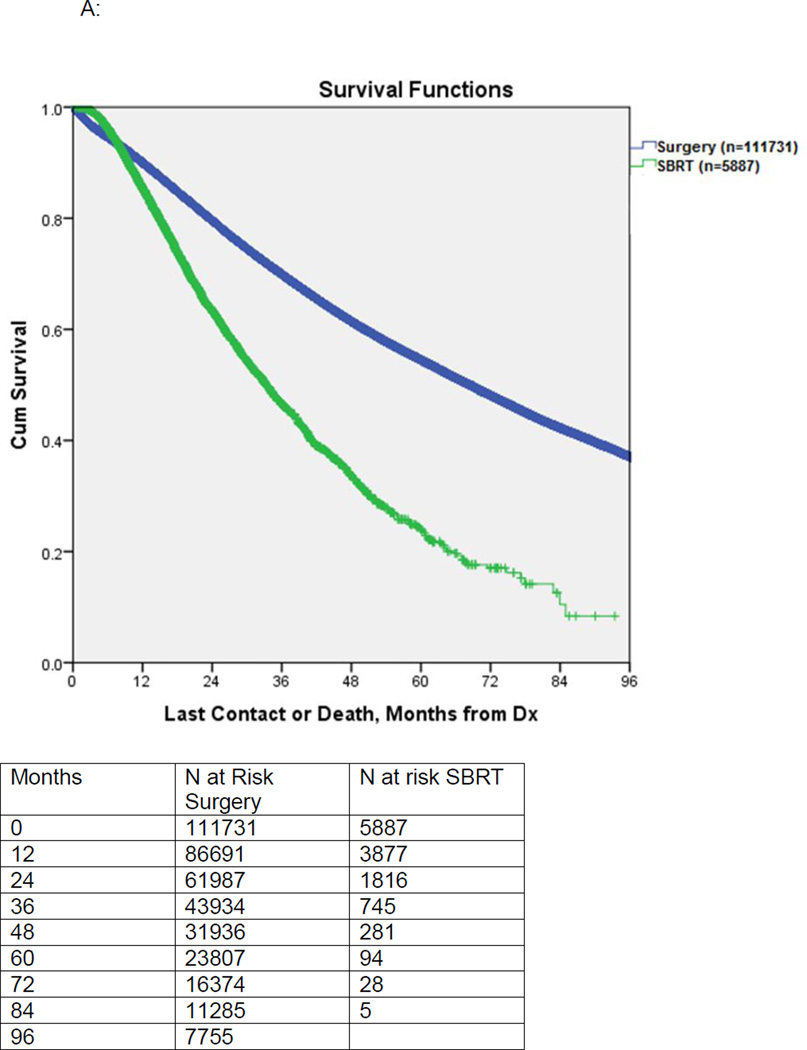
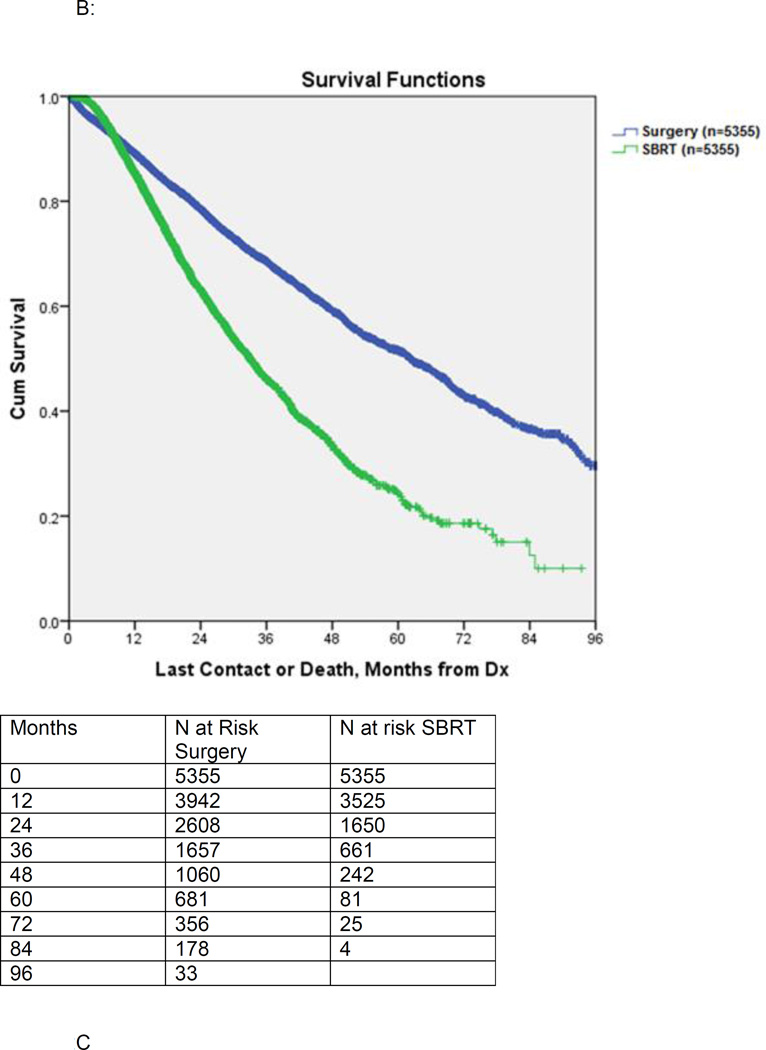
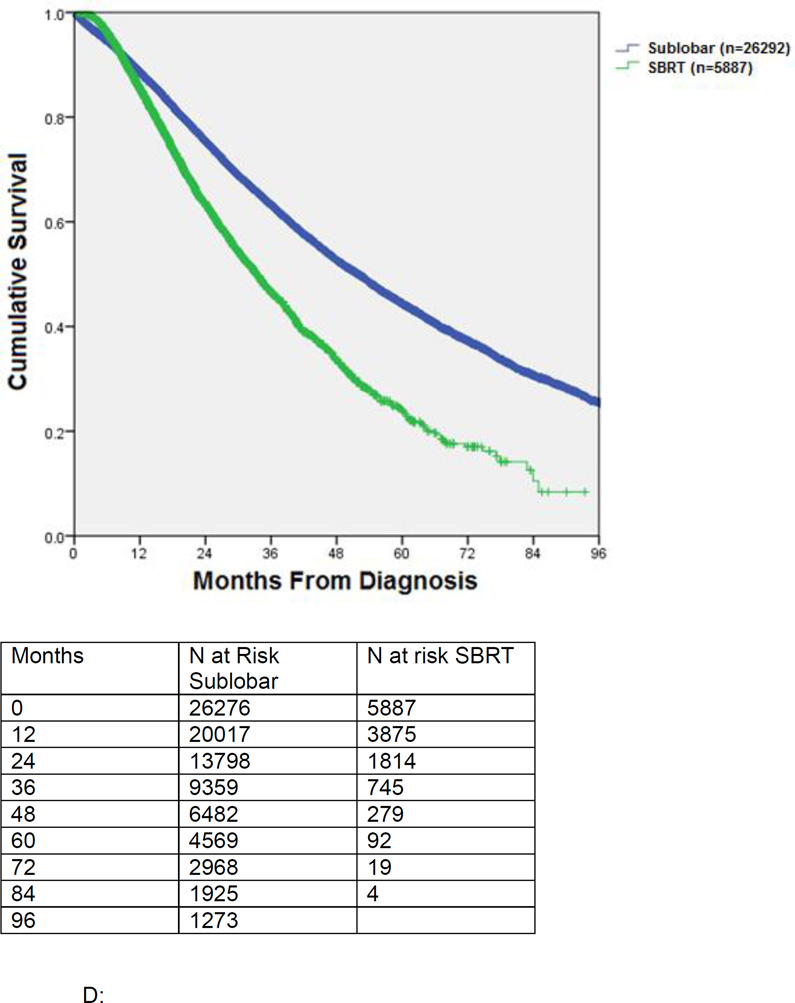
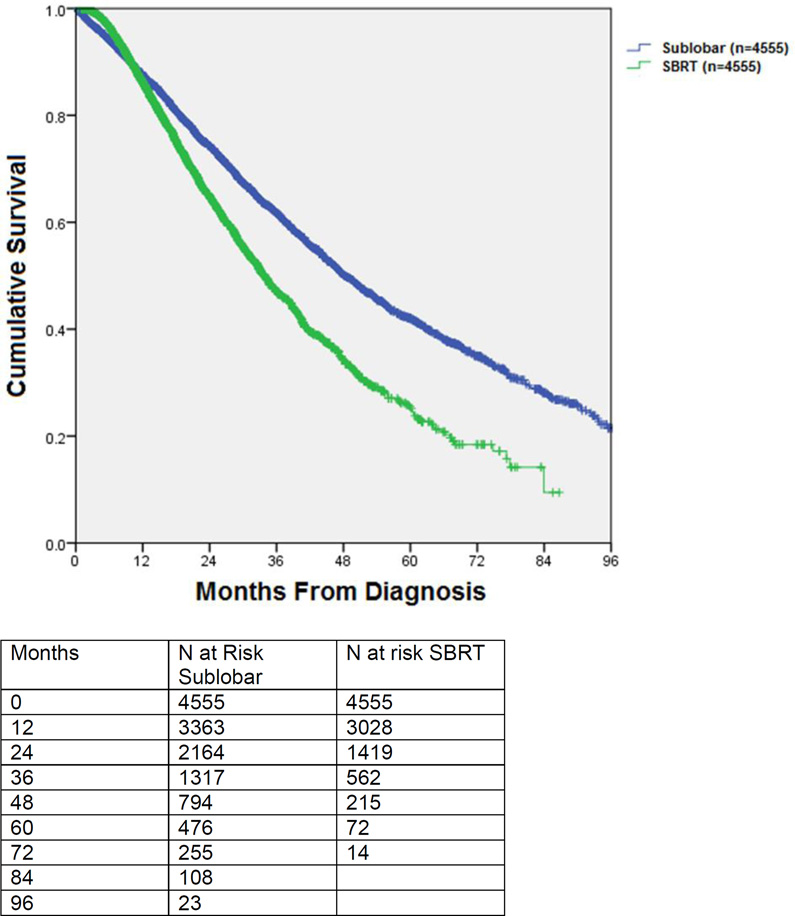
Results: Between 1998 and 2010, 117,618 patients underwent surgery or SBRT for clinical stage I NSCLC. Of these, 111,731 (95%) received surgery, whereas 5887 (5%) underwent SBRT. Patients in the surgery group were younger, more likely to be males, and had higher Charlson comorbidity scores. SBRT patients were more likely to have T1 (versus T2) tumors and receive treatment at academic centers. Thirty-day surgical mortality was 2596 of 109,485 (2.4%). Median overall survival favored the surgery group in both unmatched (68.4 versus 33.3 months, p < 0.001) and matched analysis based on patient characteristics (62.3 versus 33.1 months, p < 0.001). Disease-specific survival was unavailable from the data set.
Conclusion: In a propensity matched comparison, patients selected for surgery have improved survival compared with SBRT. In the absence of information on cause of death and with limited variables to characterize comorbidity, it is not possible to assess the relative contribution of patient selection or better cancer control toward the improved survival. Rigorous prospective studies are needed to optimize patient selection for SBRT in the high-risk surgical population.
Figures
Comment in
-
Treatment Outcomes in Stage I Lung Cancer: A Comparison of Surgery and Stereotactic Body Radiation Therapy.J Thorac Oncol. 2016 May;11(5):e64-e65. doi: 10.1016/j.jtho.2016.02.012. J Thorac Oncol. 2016. PMID: 27131296 No abstract available.
-
In Response to Treatment Outcomes in Stage I Lung Cancer: A Comparison of Surgery and Stereotactic Body Radiation Therapy.J Thorac Oncol. 2016 May;11(5):e65-e66. doi: 10.1016/j.jtho.2016.02.019. J Thorac Oncol. 2016. PMID: 27131297 No abstract available.
References
-
- Crabtree TD, Denlinger CE, Meyers BF, et al. Stereotactic body radiation therapy versus surgical resection for stage I non-small cell lung cancer. J Thorac Cardiovasc Surg. 2010;140:377–386. - PubMed
-
- Verstegen NE, Oosterhuis JW, Palma DA, et al. Stage I–II non-small-cell lung cancer treated using either stereotactic ablative radiotherapy (SABR) or lobectomy by video-assisted thoracoscopic surgery (VATS): outcomes of a propensity score-matched analysis. Ann Oncol. 2013;24:1543–1548. - PubMed
-
- Mokhles S, Verstegen N, Maat AP, et al. Comparison of clinical outcome of stage I non-small cell lung cancer treated surgically or with stereotactic radiotherapy: Results from propensity score analysis. Lung Cancer. 2015 - PubMed
-
- Varlotto J, Fakiris A, Flickinger J, et al. Matched-pair and propensity score comparisons of outcomes of patients with clinical stage I non-small cell lung cancer treated with resection or stereotactic radiosurgery. Cancer. 2013;119:2683–2691. - PubMed
-
- Lagerwaard FJ, Verstegen NE, Haasbeek CJ, et al. Outcomes of stereotactic ablative radiotherapy in patients with potentially operable stage I non-small cell lung cancer. Int J Radiat Oncol Biol Phys. 2012;83:348–353. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
