

Accuracy of [18F]FDG PET/MRI for the Detection of Liver Metastases
- PMID: 26335246
- PMCID: PMC4559465
- DOI: 10.1371/journal.pone.0137285
Accuracy of [18F]FDG PET/MRI for the Detection of Liver Metastases
Abstract
Background: The aim of this study was to compare the diagnostic accuracy of [18F]FDG-PET/MRI with PET/CT for the detection of liver metastases.
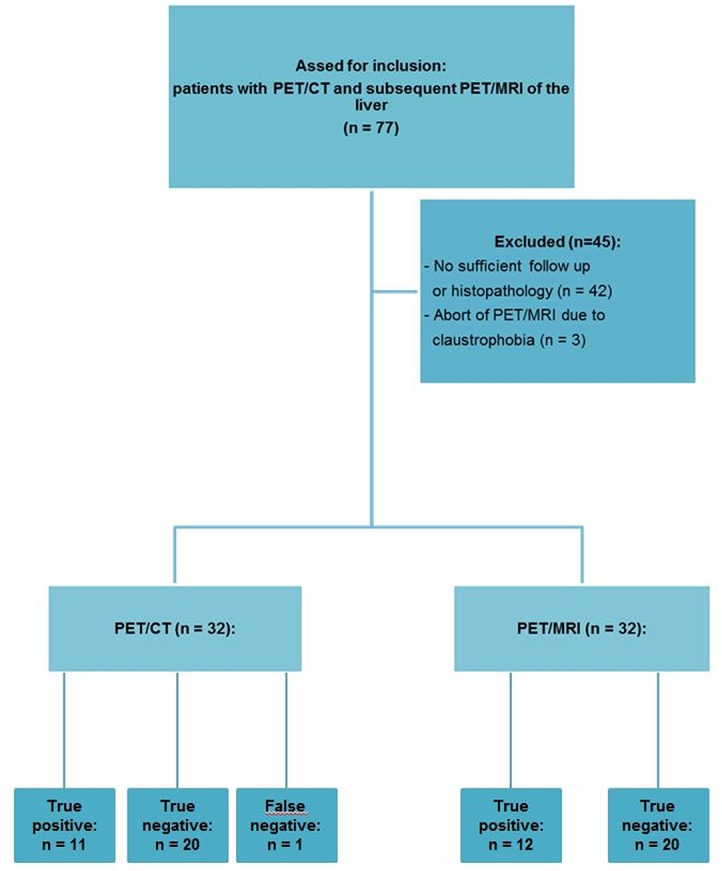
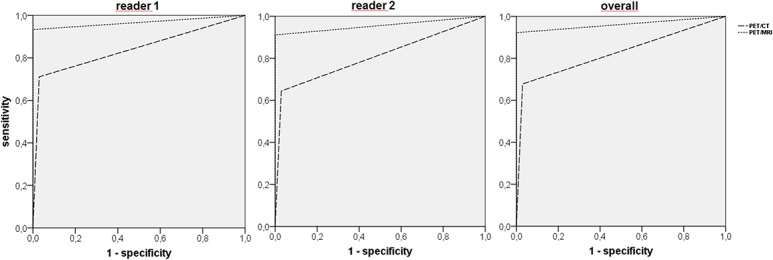
Methods: 32 patients with solid malignancies underwent [18F]FDG-PET/CT and subsequent PET/MRI of the liver. Two readers assessed both datasets regarding lesion characterization (benign, indeterminate, malignant), conspicuity and diagnostic confidence. An imaging follow-up (mean interval: 185±92 days) and/-or histopathological specimen served as standards of reference. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for both modalities. Accuracy was determined by calculating the area under the receiver operating characteristic (ROC) curve. Values of conspicuity and diagnostic confidence were compared using Wilcoxon-signed-rank test.
Results: The standard of reference revealed 113 liver lesions in 26 patients (malignant: n = 45; benign: n = 68). For PET/MRI a higher accuracy (PET/CT: 82.4%; PET/MRI: 96.1%; p<0.001) as well as sensitivity (67.8% vs. 92.2%, p<0.01) and NPV (82.0% vs. 95.1%, p<0.05) were observed. PET/MRI offered higher lesion conspicuity (PET/CT: 2.0±1.1 [median: 2; range 0-3]; PET/MRI: 2.8±0.5 [median: 3; range 0-3]; p<0.001) and diagnostic confidence (PET/CT: 2.0±0.8 [median: 2; range: 1-3]; PET/MRI 2.6±0.6 [median: 3; range: 1-3]; p<0.001). Furthermore, PET/MRI enabled the detection of additional PET-negative metastases (reader 1: 10; reader 2: 12).
Conclusions: PET/MRI offers higher diagnostic accuracy compared to PET/CT for the detection of liver metastases.
Conflict of interest statement
Figures
Similar articles
-
Value of retrospective fusion of PET and MR images in detection of hepatic metastases: comparison with 18F-FDG PET/CT and Gd-EOB-DTPA-enhanced MRI.J Nucl Med. 2010 May;51(5):692-9. doi: 10.2967/jnumed.109.068510. Epub 2010 Apr 15. J Nucl Med. 2010. PMID: 20395324
-
Gadoxetate disodium-enhanced magnetic resonance imaging versus contrast-enhanced 18F-fluorodeoxyglucose positron emission tomography/computed tomography for the detection of colorectal liver metastases.Invest Radiol. 2011 Sep;46(9):548-55. doi: 10.1097/RLI.0b013e31821a2163. Invest Radiol. 2011. PMID: 21577131
-
"One-stop-shop" staging: should we prefer FDG-PET/CT or MRI for the detection of bone metastases?Eur J Radiol. 2011 Jun;78(3):430-5. doi: 10.1016/j.ejrad.2009.10.031. Epub 2009 Nov 27. Eur J Radiol. 2011. PMID: 19945240
-
Hybrid imaging for detection of carcinoma of unknown primary: A preliminary comparison trial of whole-body PET/MRI versus PET/CT.Eur J Radiol. 2016 Nov;85(11):1941-1947. doi: 10.1016/j.ejrad.2016.08.020. Epub 2016 Aug 31. Eur J Radiol. 2016. PMID: 27776644
-
Preoperative imaging of colorectal liver metastases after neoadjuvant chemotherapy: a meta-analysis.Ann Surg Oncol. 2012 Sep;19(9):2805-13. doi: 10.1245/s10434-012-2300-z. Epub 2012 Mar 7. Ann Surg Oncol. 2012. PMID: 22396005 Free PMC article. Review.
Cited by
-
Diagnostic performance of [18F]FDG-PET/MRI for liver metastasis in patients with primary malignancy: a systematic review and meta-analysis.Eur Radiol. 2019 Jul;29(7):3553-3563. doi: 10.1007/s00330-018-5909-x. Epub 2019 Feb 4. Eur Radiol. 2019. PMID: 30715585
-
International EANM-SNMMI-ISMRM consensus recommendation for PET/MRI in oncology.Eur J Nucl Med Mol Imaging. 2023 Oct;50(12):3513-3537. doi: 10.1007/s00259-023-06406-x. Epub 2023 Aug 25. Eur J Nucl Med Mol Imaging. 2023. PMID: 37624384 Free PMC article.
-
Comparative study of total-body PET and PET/MR in the diagnosis of liver metastases.Front Oncol. 2025 May 14;15:1519107. doi: 10.3389/fonc.2025.1519107. eCollection 2025. Front Oncol. 2025. PMID: 40438693 Free PMC article.
-
[Hybrid imaging of the abdomen and pelvis. German version].Radiologe. 2020 May;60(5):394-404. doi: 10.1007/s00117-020-00660-y. Radiologe. 2020. PMID: 32232543 Review. German.
-
Cost-effectiveness analysis of MRI, CE-CT and 18F-FDG PET/CT for detecting colorectal liver metastases eligible for hepatic resection.Front Oncol. 2023 Jul 24;13:1161738. doi: 10.3389/fonc.2023.1161738. eCollection 2023. Front Oncol. 2023. PMID: 37554160 Free PMC article.
References
-
- Sutherland LM, Williams JAR, Padbury RTA, Gotley DC, Stokes B, Maddern GJ et al. (2006) Radiofrequency ablation of liver tumors: a systematic review. Arch Surg 141 (2): 181–190. - PubMed
-
- Scharitzer M, Ba-Ssalamah A, Ringl H, Kolblinger C, Grunberger T, Weber M et al. (2013) Preoperative evaluation of colorectal liver metastases: comparison between gadoxetic acid-enhanced 3.0-T MRI and contrast-enhanced MDCT with histopathological correlation. Eur Radiol 23 (8): 2187–2196. 10.1007/s00330-013-2824-z - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
