

Access to specialist care: Optimizing the geographic configuration of trauma systems
- PMID: 26335775
- PMCID: PMC4623849
- DOI: 10.1097/TA.0000000000000827
Access to specialist care: Optimizing the geographic configuration of trauma systems
Abstract
Background: The optimal geographic configuration of health care systems is key to maximizing accessibility while promoting the efficient use of resources. This article reports the use of a novel approach to inform the optimal configuration of a national trauma system.
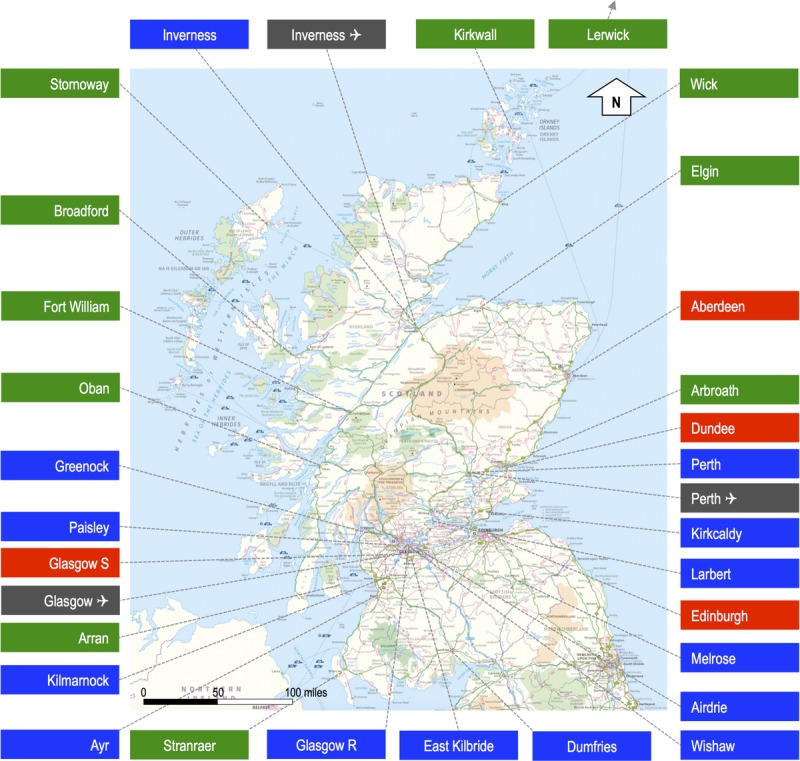
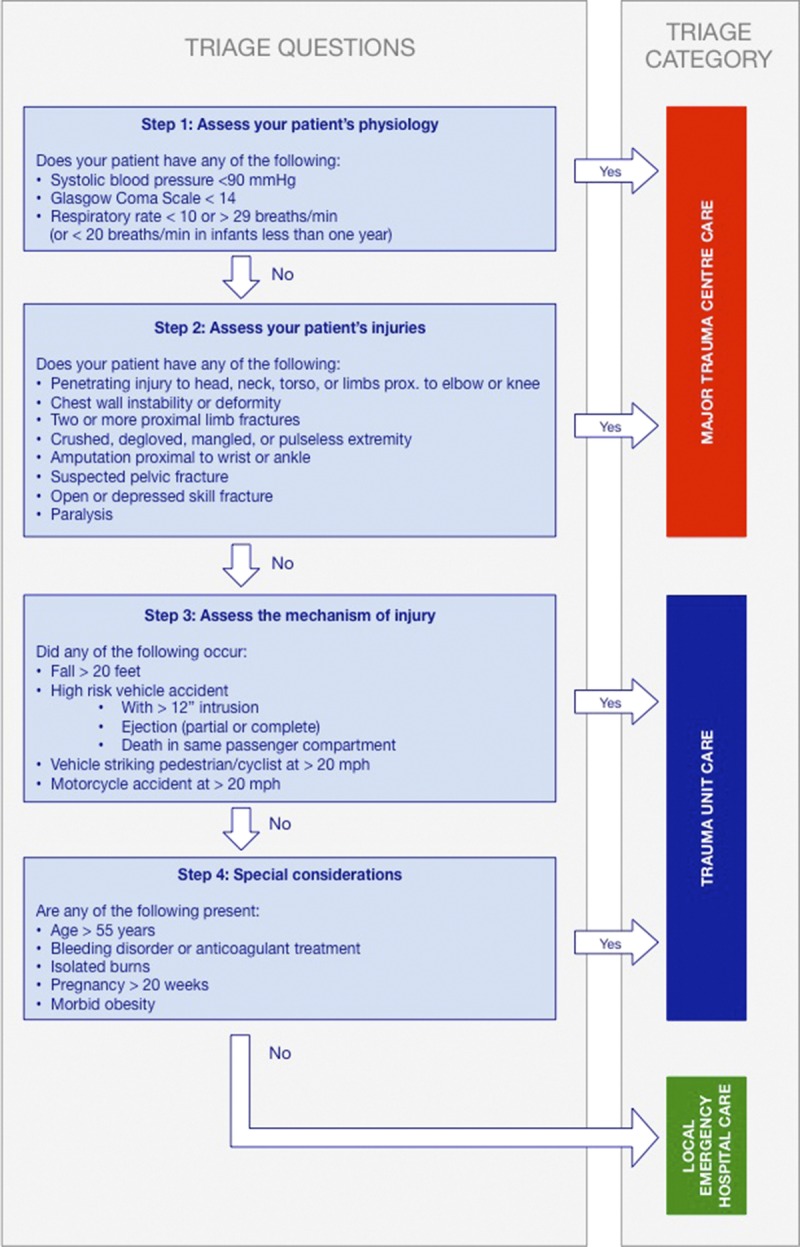
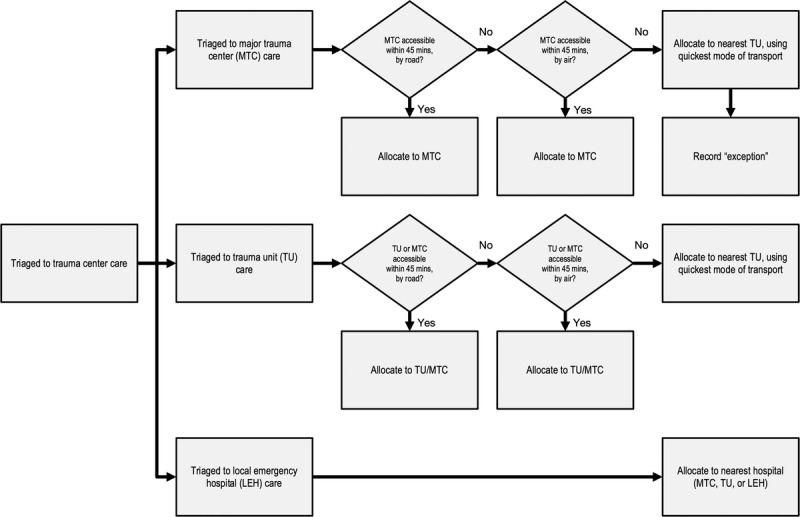
Methods: This is a prospective cohort study of all trauma patients, 15 years and older, attended to by the Scottish Ambulance Service, between July 1, 2013, and June 30, 2014. Patients underwent notional triage to one of three levels of care (major trauma center [MTC], trauma unit, or local emergency hospital). We used geographic information systems software to calculate access times, by road and air, from all incident locations to all candidate hospitals. We then modeled the performance of all mathematically possible network configurations and used multiobjective optimization to determine geospatially optimized configurations.
Results: A total of 80,391 casualties were included. A network with only high- or moderate-volume MTCs (admitting at least 650 or 400 severely injured patients per year, respectively) would be optimally configured with a single MTC. A network accepting lower-volume MTCs (at least 240 severely injured patients per year) would be optimally configured with two MTCs. Both configurations would necessitate an increase in the number of helicopter retrievals.
Conclusion: This study has shown that a novel combination of notional triage, network analysis, and mathematical optimization can be used to inform the planning of a national clinical network. Scotland's trauma system could be optimized with one or two MTCs.
Level of evidence: Care management study, level IV.
Figures
Comment in
-
Analysis of aeromedical retrieval coverage using elliptical isochrones.J Trauma Acute Care Surg. 2017 Jun;82(6):1186-1187. doi: 10.1097/TA.0000000000001457. J Trauma Acute Care Surg. 2017. PMID: 28328678 No abstract available.
-
Re: Analysis of aeromedical retrieval coverage using elliptical isochrones.J Trauma Acute Care Surg. 2017 Jun;82(6):1187. doi: 10.1097/TA.0000000000001458. J Trauma Acute Care Surg. 2017. PMID: 28328680 No abstract available.
References
-
- Gabbe BJ, Simpson PM, Sutherland AM, Wolfe R, Fitzgerald MC, Judson R, Cameron PA. Improved functional outcomes for major trauma patients in a regionalized, inclusive trauma system. Ann Surg. 2012; 255(6): 1009– 1015. - PubMed
-
- MacKenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Frey KP, Egleston BL, Salkever DS, Scharfstein DO. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006; 354(4): 366– 378. - PubMed
-
- Mackenzie EJ, Rivara FP, Jurkovich GJ, Nathens AB, Egleston BL, Salkever DS, Frey KP, Scharfstein DO. The impact of trauma-center care on functional outcomes following major lower-limb trauma. J Bone Joint Surg Am. 2008; 90(1): 101– 109. - PubMed
-
- American College of Surgeons Committee on Trauma. Resources for Optimal Care of the. Chicago, IL; American College of Surgeons; 2006.
-
- Markovchick VJ, Moore EE. Optimal trauma outcome: trauma system design and the trauma team. Emerg Med Clin North Am. 2007; 25(3): 643– 654. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
