

Prognostic value of Tpeak-Tend interval in patients with acute pulmonary embolism
- PMID: 26335802
- PMCID: PMC4557924
- DOI: 10.1186/s12872-015-0091-4
Prognostic value of Tpeak-Tend interval in patients with acute pulmonary embolism
Abstract
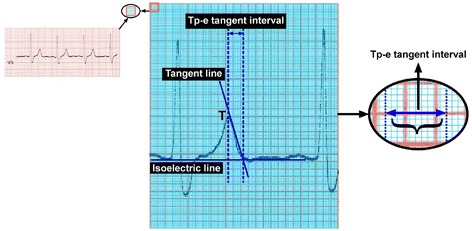
Background: The aim of this study was to examine the Tpeak-Tend (Tpe/corrected Tpe) interval, which is an indicator of transmural myocardial repolarization, measured non-invasively via electrocardiogram in patients with acute pulmonary embolism (PE), and to investigate the relationship with 30-day mortality and morbidity.
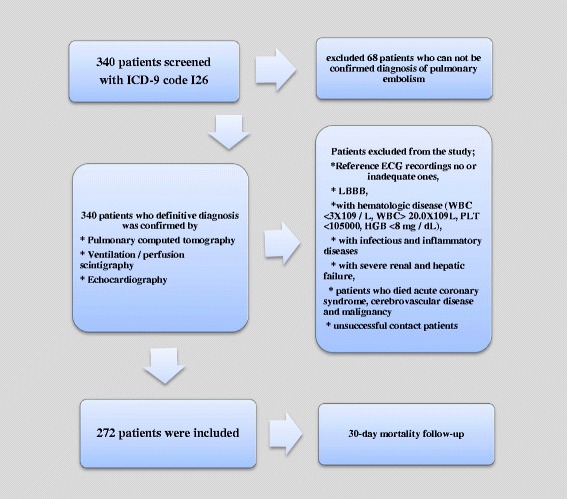
Methods: The study included 272 patients diagnosed with acute PE, comprising 154 females and 118 males, with a mean age of 63.1 ± 16.8 years. Tpe/cTpe intervals were calculated from the electrocardiograms with a computer program after using a ruler or vernier caliper manual measuring tool to obtain highly sensitive measurements. The relationship between the electrocardiogram values and 30-days mortality and morbidity were measured.
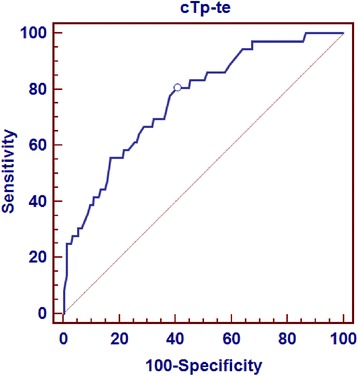
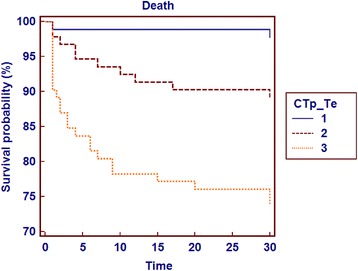
Results: The study group was divided into three groups according to cTpe intervals: Group 1, < 113 ms; Group 2, 113-133 ms; and Group 3, > 133 ms. White blood cell count and troponin T levels, corrected QT intervals with QRS complex durations, percentage of right ventricle dilatation with right/left-ventricular ratio, 30-day death, and combinations of these values were seen at a higher rate in Group 3 patients compared to the other groups. Kaplan-Meier analysis showed that the cTpe interval measured at > 126 ms could be used as a cut-off value in the prediction of mortality and morbidity. The cTpe cut-off values of 126 ms had sensivity, specificity, negative predictive value, and positive predictive value of 80.56 %, 59.32 %, 95.2 %, and 23.2 %, respectively.
Conclusions: cTpe interval could be a useful method in early risk stratification in patients with acute PE.
Figures
Similar articles
-
Combined risk stratification with computerized tomography /echocardiography and biomarkers in patients with normotensive pulmonary embolism.Thromb Res. 2010 Dec;126(6):486-92. doi: 10.1016/j.thromres.2010.08.021. Thromb Res. 2010. PMID: 20920821
-
Prognostic significance of PaO2/PaCO2 ratio in normotensive patients with pulmonary embolism.Clin Respir J. 2012 Apr;6(2):104-11. doi: 10.1111/j.1752-699X.2011.00253.x. Epub 2011 Jul 19. Clin Respir J. 2012. PMID: 21651744
-
Tpeak-to-Tend interval corrected for heart rate: A more precise measure of increased sudden death risk?Heart Rhythm. 2016 Nov;13(11):2181-2185. doi: 10.1016/j.hrthm.2016.08.022. Epub 2016 Aug 11. Heart Rhythm. 2016. PMID: 27523774 Free PMC article.
-
Increased Tpeak-Tend interval is highly and independently related to arrhythmic events in Brugada syndrome.Heart Rhythm. 2015 Dec;12(12):2469-76. doi: 10.1016/j.hrthm.2015.07.029. Epub 2015 Jul 21. Heart Rhythm. 2015. PMID: 26209263
-
CT signs of right ventricular dysfunction: prognostic role in acute pulmonary embolism.JACC Cardiovasc Imaging. 2011 Aug;4(8):841-9. doi: 10.1016/j.jcmg.2011.04.013. JACC Cardiovasc Imaging. 2011. PMID: 21835376
Cited by
-
A Longer Tpeak-Tend Interval Is Associated with a Higher Risk of Death: A Meta-Analysis.J Clin Med. 2023 Jan 28;12(3):992. doi: 10.3390/jcm12030992. J Clin Med. 2023. PMID: 36769640 Free PMC article. Review.
-
Diagnostic value of the corrected QT difference between leads V1 and V6 in patients with acute pulmonary thromboembolism.Medicine (Baltimore). 2017 Oct;96(43):e8430. doi: 10.1097/MD.0000000000008430. Medicine (Baltimore). 2017. PMID: 29069044 Free PMC article.
-
Is there a relationship between epicardial fat tissue thickness and Tp-Te/QT ratio in healthy individuals?Arch Med Sci Atheroscler Dis. 2020 Jun 5;5:e127-e139. doi: 10.5114/aoms.2020.96147. eCollection 2020. Arch Med Sci Atheroscler Dis. 2020. PMID: 32665987 Free PMC article.
-
Effect of pulmonary embolism location on electrocardiological parameters.Rev Assoc Med Bras (1992). 2023 Nov 13;69(12):e20230733. doi: 10.1590/1806-9282.20230733. eCollection 2023. Rev Assoc Med Bras (1992). 2023. PMID: 37971127 Free PMC article.
-
Evaluation of TP-E Interval and TP-E/QT Ratio in Panic Disorder.Medicina (Kaunas). 2020 Apr 28;56(5):215. doi: 10.3390/medicina56050215. Medicina (Kaunas). 2020. PMID: 32353958 Free PMC article.
References
-
- Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. Guidelines on diagnosis and management of acute pulmonary embolism. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism: The Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Endorsed by the European Respiratory Society (ERS) Eur Heart J. 2014;35(43):3033–3073. doi: 10.1093/eurheartj/ehu283. - DOI - PubMed
-
- Laporte S, Mismetti P, De’cousus H, Uresandi F, Otero R, Lobo JL, et al. Clinical predictors for fatal pulmonary embolism in 15,520 patients with venous thromboembolism: Findings from the Registro Informatizado de la Enfermedad Trombo Embolicavenosa (RIETE) Registry. Circulation. 2008;117(13):1711–1716. doi: 10.1161/CIRCULATIONAHA.107.726232. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
