

Noninvasive pulse pressure variation and stroke volume variation to predict fluid responsiveness at multiple thresholds: a prospective observational study
- PMID: 26335905
- PMCID: PMC4595532
- DOI: 10.1007/s12630-015-0464-2
Noninvasive pulse pressure variation and stroke volume variation to predict fluid responsiveness at multiple thresholds: a prospective observational study
Abstract
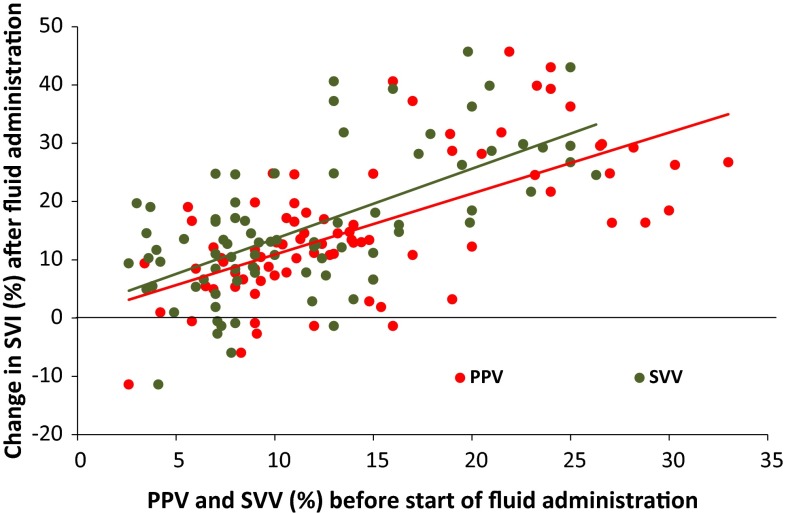
Background: Pulse pressure variation (PPV) and stroke volume variation (SVV) are dynamic preload variables that can be measured noninvasively to assess fluid responsiveness (FR) in anesthetized patients with mechanical ventilation. Few studies have examined the effectiveness of predicting FR according to the definition of FR, and assessment of inconclusive values of PPV and SVV around the cut-off value (the "grey zone") might improve individual FR prediction. We explored the ability of noninvasive volume clamp derived measurements of PPV and SVV to predict FR using the grey zone approach, and we assessed the influence of multiple thresholds on the predictive ability of the numerical definition of FR.
Methods: Ninety patients undergoing general surgery were included in this prospective observational study and received a 500 mL fluid bolus as deemed clinically required by the attending anesthesiologist. A minimal relative increase in stroke volume index (↑SVI) was used to define FR with different thresholds from 10-25%. The PPV, SVV, and SVI were measured using the Nexfin® device that employs noninvasive volume clamp plethysmography.
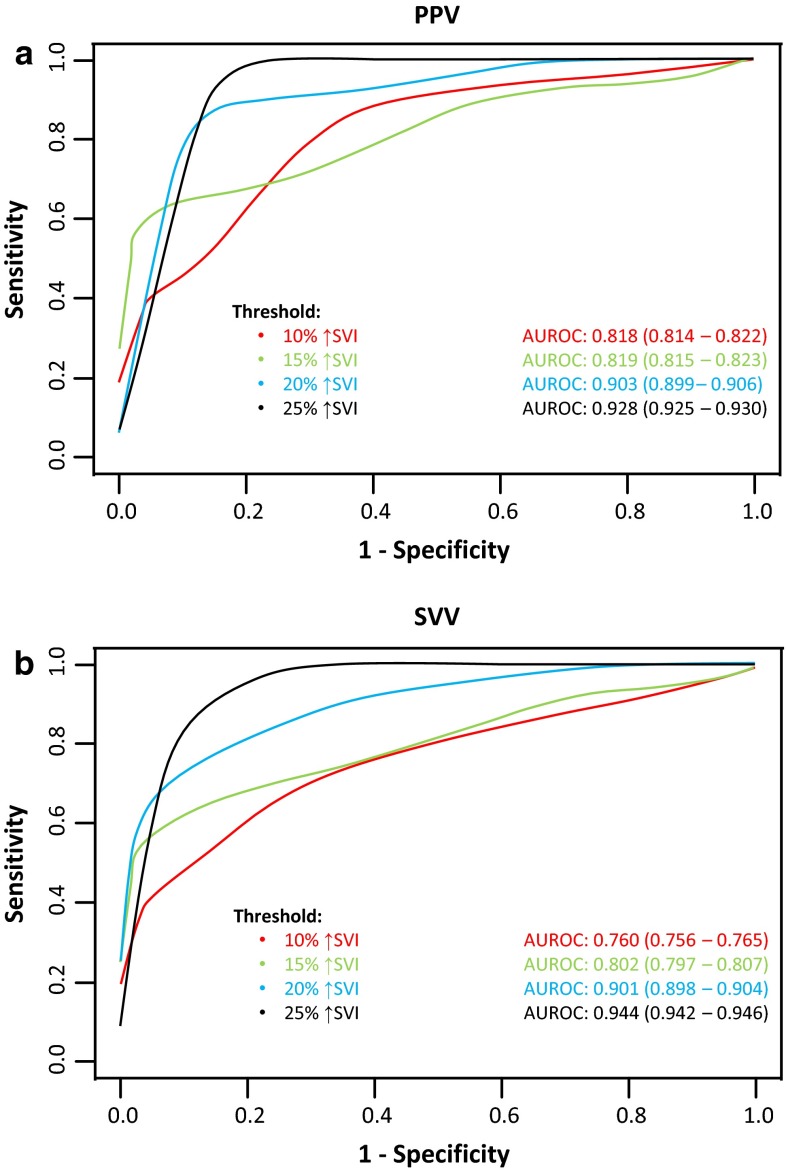
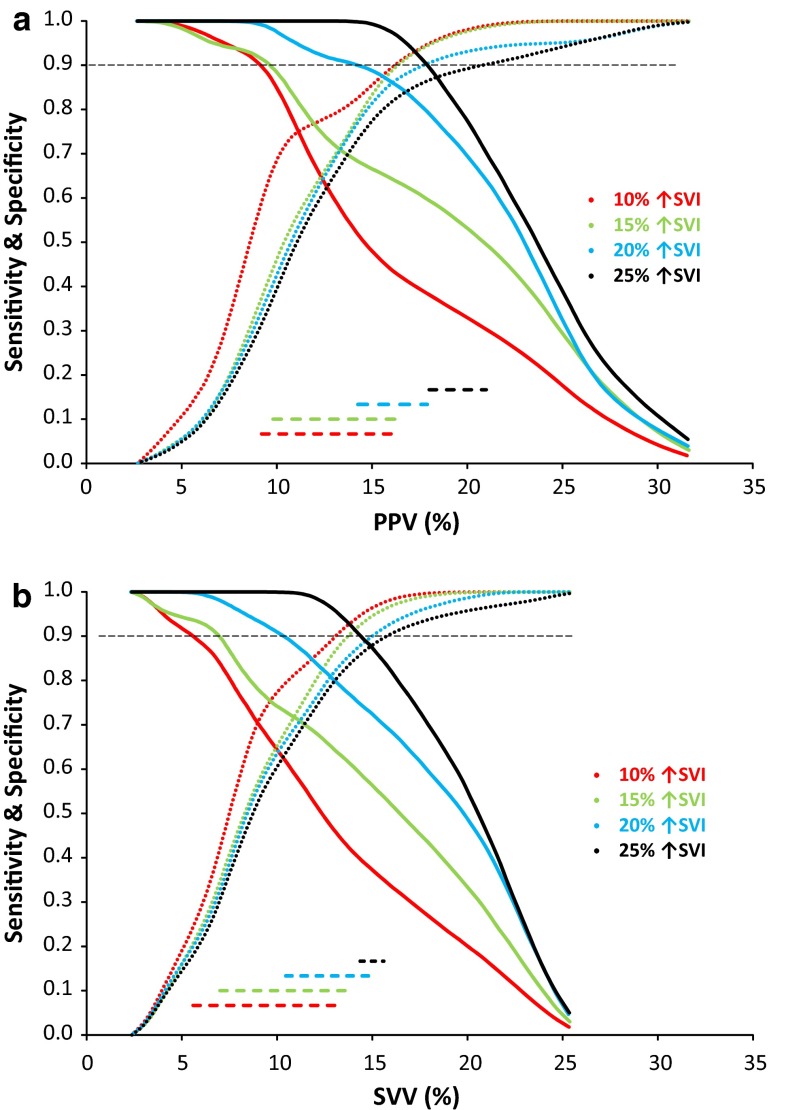
Results: The area under the receiver operator characteristic curve gradually increased for PPV / SVV with higher threshold values (from 0.818 / 0.760 at 10% ↑SVI to 0.928 / 0.944 at 25% ↑SVI). The grey zone limits of both PPV and SVV changed from 9-16% (PPV) and 5-13% (SVV) at the 10% ↑SVI threshold to 18-21% (PPV) and 14-16% (SVV) at the 25% ↑SVI threshold.
Conclusion: Noninvasive PPV and SVV measurements allow an acceptable FR prediction, although the reliability of both variables is dependent on the intended increase in SVI, which improves substantially with concomitant smaller grey zones at higher ↑SVI thresholds.
Contexte: La variation de pression différentielle (VPD) et la variation de volume d’éjection (VVE) sont des variables de précharge dynamiques qui peuvent être mesurées de façon non invasive afin d’évaluer la réponse liquidienne (RL) chez les patients anesthésiés sous ventilation mécanique. Peu d’études ont examiné l’efficacité de prédire la RL selon la valeur prédéterminée d’interruption du traitement, et l’évaluation de valeurs non concluantes de VPD et de VVE (la « zone grise ») pourrait améliorer la prédiction de la RL individuelle. Nous avons exploré l’utilisation de la méthode à volume imposé (« volume clamp method ») pour les mesures non invasives de la VPD et de la VVE afin de prédire la RL en utilisant l’approche de zone grise, et nous avons évalué l’influence de plusieurs seuils sur la capacité prédictive de la définition numérique de la RL.
Méthode: Quatre-vingt dix patients subissant une chirurgie générale ont été inclus dans cette étude observationnelle prospective et ont reçu un bolus liquidien de 500 mL lorsque l’anesthésiologiste en charge a jugé le bolus était nécessaire d’un point de vue clinique. Une augmentation relative minimale de l’indice de volume d’éjection (↑IVE) a été utilisée pour définir la RL avec différents seuils allant de 10 à 25 %. Les VPD, VVE et IVE ont été mesurés à l’aide d’un dispositif Nexfin® qui se fonde sur une pléthysmographie à volume imposé non invasive.
Résultats: La surface sous la courbe ROC a progressivement augmenté pour la VPD et la VVE avec des valeurs seuils plus élevées (de 0,818 / 0,760 à 10 % ↑IVE à 0,928 / 0,944 à 25 % ↑IVE). Les limites de zone grise de la VPD et de la VVE ont changé lorsqu’on a atteint le seuil de 10 % ↑IVE (de 9-16 % et 5-13 %, respectivement) et au seuil de 25 % ↑IVE (de 18-21 % et 14-16 %, respectivement).
Conclusion: Les mesures non invasives de la VPD et de la VVE permettent de prédire de façon acceptable la RL, bien que la fiabilité de ces deux variables dépende de l’augmentation prévue de l’IVE, qui s’améliore considérablement avec des zones grises concomitantes plus petites à des seuils plus élevés d’↑IVE.
Electronic supplementary material: The online version of this article (doi:10.1007/s12630-015-0464-2) contains supplementary material, which is available to authorized users.
Figures
Comment in
-
The "grey zone" or how to avoid the binary constraint of decision-making.Can J Anaesth. 2015 Nov;62(11):1139-42. doi: 10.1007/s12630-015-0465-1. Epub 2015 Aug 22. Can J Anaesth. 2015. PMID: 26296301 No abstract available.
Similar articles
-
Non-invasive measurements of pulse pressure variation and stroke volume variation in anesthetized patients using the Nexfin blood pressure monitor.J Clin Monit Comput. 2016 Oct;30(5):587-94. doi: 10.1007/s10877-015-9759-7. Epub 2015 Aug 29. J Clin Monit Comput. 2016. PMID: 26318314 Free PMC article.
-
Stroke volume and pulse pressure variation for prediction of fluid responsiveness in patients undergoing off-pump coronary artery bypass grafting.Chest. 2005 Aug;128(2):848-54. doi: 10.1378/chest.128.2.848. Chest. 2005. PMID: 16100177 Clinical Trial.
-
[Stroke volume and pulse pressure variation are good predictors of fluid responsiveness in sepsis patients].Acta Med Croatica. 2013 Dec;67(5):407-14. Acta Med Croatica. 2013. PMID: 24979881 Croatian.
-
Reliability of pulse pressure and stroke volume variation in assessing fluid responsiveness in the operating room: a metanalysis and a metaregression.Crit Care. 2023 Nov 8;27(1):431. doi: 10.1186/s13054-023-04706-0. Crit Care. 2023. PMID: 37940953 Free PMC article.
-
A systematic review of pulse pressure variation and stroke volume variation to predict fluid responsiveness during cardiac and thoracic surgery.J Clin Monit Comput. 2017 Aug;31(4):677-684. doi: 10.1007/s10877-016-9898-5. Epub 2016 Jun 15. J Clin Monit Comput. 2017. PMID: 27306799
Cited by
-
Comparison of Noninvasive Dynamic Indices of Fluid Responsiveness Among Different Ventilation Modes in Dogs Recovering from Experimental Cardiac Surgery.Med Sci Monit. 2018 Oct 29;24:7736-7741. doi: 10.12659/MSM.910135. Med Sci Monit. 2018. PMID: 30372425 Free PMC article.
-
Comparison of the carotid corrected flow time and tidal volume challenge for assessing fluid responsiveness in robot-assisted laparoscopic surgery.J Robot Surg. 2023 Dec;17(6):2763-2772. doi: 10.1007/s11701-023-01710-y. Epub 2023 Sep 14. J Robot Surg. 2023. PMID: 37707743 Clinical Trial.
-
Effects of goal-directed fluid management guided by a non-invasive device on the incidence of postoperative complications in neurosurgery: a pilot and feasibility randomized controlled trial.Perioper Med (Lond). 2023 Jul 5;12(1):32. doi: 10.1186/s13741-023-00321-3. Perioper Med (Lond). 2023. PMID: 37408018 Free PMC article.
-
Novel noninvasive prediction for pulse pressure variation: a machine learning-based model.Br J Anaesth. 2025 Apr;134(4):1200-1203. doi: 10.1016/j.bja.2024.12.028. Epub 2025 Jan 24. Br J Anaesth. 2025. PMID: 39863466 Free PMC article. No abstract available.
-
The Impact of Individualized Hemodynamic Management on Intraoperative Fluid Balance and Hemodynamic Interventions during Spine Surgery in the Prone Position: A Prospective Randomized Trial.Medicina (Kaunas). 2022 Nov 20;58(11):1683. doi: 10.3390/medicina58111683. Medicina (Kaunas). 2022. PMID: 36422222 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
