

Comprehensive Genomic Profiling of Advanced Esophageal Squamous Cell Carcinomas and Esophageal Adenocarcinomas Reveals Similarities and Differences
- PMID: 26336083
- PMCID: PMC4591943
- DOI: 10.1634/theoncologist.2015-0156
Comprehensive Genomic Profiling of Advanced Esophageal Squamous Cell Carcinomas and Esophageal Adenocarcinomas Reveals Similarities and Differences
Abstract
Background: Esophageal squamous cell carcinomas (ESCCs) and esophageal adenocarcinomas (EACs) account for >95% of esophageal malignancies and represent a major global health burden. ESCC is the dominant histology globally but represents a minority of U.S. cases, with EAC accounting for the majority of U.S.
Cases: The patient outcomes for advanced ESCC and EAC are poor, and new therapeutic options are needed. Using a sensitive sequencing assay, we compared the genomic profiles of ESCC and EAC with attention to identification of therapeutically relevant genomic alterations.
Methods: Next-generation sequencing-based comprehensive genomic profiling was performed on hybridization-captured, adaptor ligation-based libraries to a median coverage depth of >650× for all coding exons of 315 cancer-related genes plus selected introns from 28 genes frequently rearranged in cancer. Results from a single sample were evaluated for all classes of genomic alterations (GAs) including point mutations, short insertions and deletions, gene amplifications, homozygous deletions, and fusions/rearrangements. Clinically relevant genomic alterations (CRGAs) were defined as alterations linked to approved drugs and those under evaluation in mechanism-driven clinical trials.
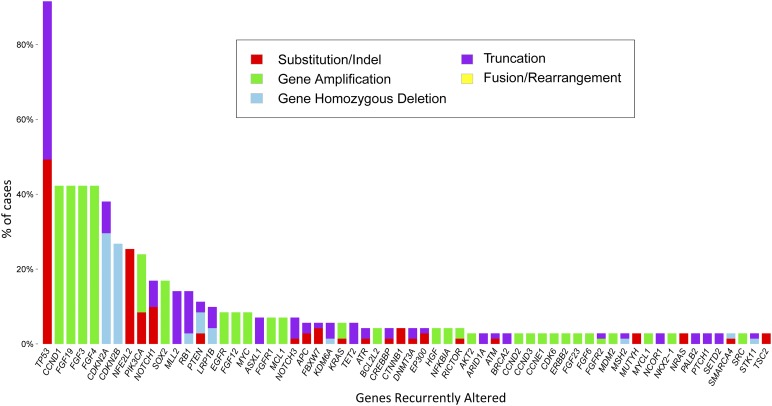
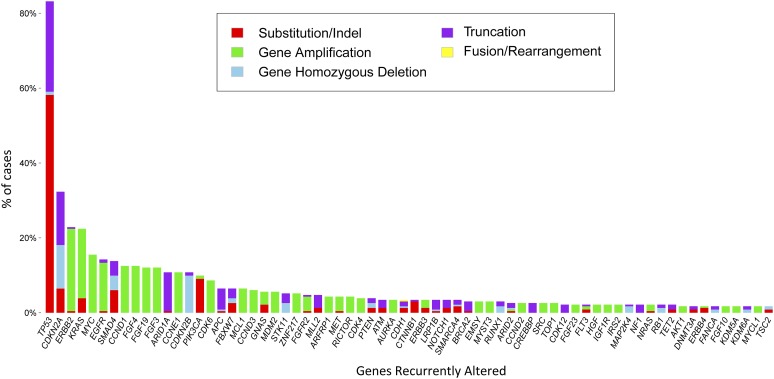
Results: There were no significant differences by sex for either tumor type, and the median age for all patients was 63 years. All ESCCs and EACs were at an advanced stage at the time of sequencing. All 71 ESCCs and 231 EACs featured GAs on profiling, with 522 GAs in ESCC (7.4 per sample) and 1,303 GAs in EAC (5.6 per sample). The frequency of clinically relevant GAs in ESCC was 94% (2.6 per sample) and 93% in EAC (2.7 per sample). CRGAs occurring more frequently in EAC included KRAS (23% EAC vs. 6% ESCC) and ERBB2 (23% EAC vs. 3% ESCC). ESCC samples were enriched for CRGA in PIK3CA (24% ESCC vs. 10% EAC), PTEN (11% ESCC vs. 4% EAC), and NOTCH1 (17% ESCC vs. 3% EAC). Other GAs that differed significantly between histologic tumor types included SMAD4 (14% EAC vs. 1% ESCC), RB1 (14% ESCC vs. 2% EAC), SOX2 (18% ESCC vs. 1% EAC), and NFE2L2 (24% ESCC vs. 1% EAC).
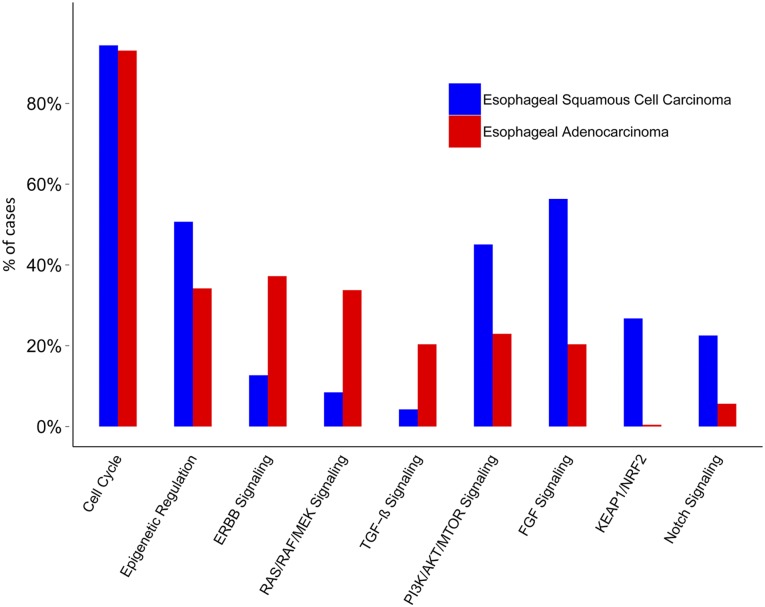
Conclusion: ESCC and EAC share similarly high frequencies of overall and clinically relevant genomic alterations; however, the profiles of genomic alterations in the two diseases differ widely, with KRAS and ERBB2 far more frequently altered in EAC compared with ESCC and with mammalian target of rapamycin (MTOR) pathway genes (PIK3CA and PTEN) and NOTCH1 more frequently altered in ESCC compared with EAC. Comprehensive genomic profiling highlights the promise of identifying clinically relevant genomic alterations in both ESCC and EAC and suggests new avenues for molecularly directed therapies in esophageal cancer.
Keywords: Adenocarcinoma; Comprehensive genomic profiling; Esophageal cancer; Next-generation sequencing; Squamous cell; Targeted therapy.
©AlphaMed Press.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349:2241–2252. - PubMed
-
- Engel LS, Chow WH, Vaughan TL, et al. Population attributable risks of esophageal and gastric cancers. J Natl Cancer Inst. 2003;95:1404–1413. - PubMed
-
- Lagergren J, Lagergren P. Recent developments in esophageal adenocarcinoma. CA Cancer J Clin. 2013;63:232–248. - PubMed
-
- Pennathur A, Gibson MK, Jobe BA, et al. Oesophageal carcinoma. Lancet. 2013;381:400–412. - PubMed
-
- Al-Haddad S, El-Zimaity H, Hafezi-Bakhtiari S, et al. Infection and esophageal cancer. Ann N Y Acad Sci. 2014;1325:187–196. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
