

Measurement of the ventriculoatrial interval from the coronary sinus during para-Hisian pacing may fail to distinguish ventriculoatrial nodal conduction from conduction over a septal accessory pathway
- PMID: 26336521
- PMCID: PMC4550193
- DOI: 10.1016/j.joa.2014.05.005
Measurement of the ventriculoatrial interval from the coronary sinus during para-Hisian pacing may fail to distinguish ventriculoatrial nodal conduction from conduction over a septal accessory pathway
Abstract
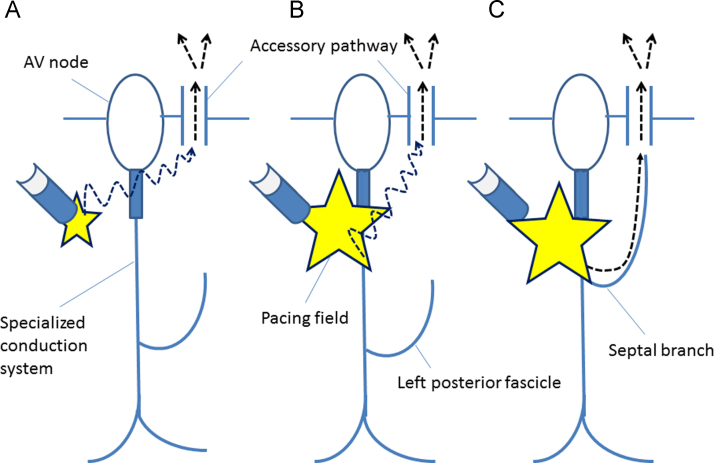
Background: Para-Hisian pacing (PHP) helps differentiate retrograde conduction over an accessory pathway (AP) from retrograde conduction over the atrioventricular (AV) node. This study examined a potential limitation of this technique, focusing on the measurement of the ventriculoatrial (V-A) interval from the coronary sinus (CS) during PHP.
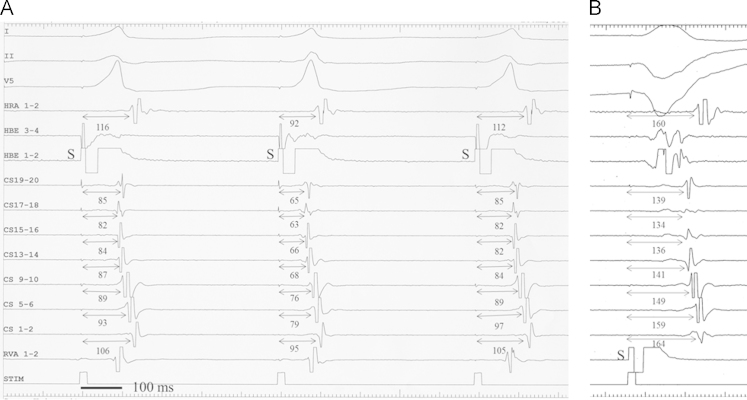
Methods: Our subjects were 9 patients undergoing electrophysiological studies before successful catheter ablation of a posteroseptal AP. During PHP, retrograde conduction occurred over an AP when the pacing stimulus to atrium (S-A) interval recorded near the AP remained unchanged whether the His bundle (HB) was captured or not (pattern 1), or when a loss of HB capture was associated with an increase in the S-A interval and no change in the V-A interval near the AP (pattern 2).
Results: Patterns 1 and 2 were observed in 5 (56%) and 2 (22%) patients, respectively. However, in the remaining 2 patients (22%), loss of HB capture during PHP was associated with an increase in the S-A interval (as in pattern 2), whereas the V-A interval near the AP could not be measured because no ventricular electrogram was visible on the CS recording (pattern 3); therefore, the presence of AP could not be confirmed by PHP. In patterns 2 and 3, the atrial activation sequence remained unchanged whether the HB was captured or not.
Conclusions: PHP may not be able to discriminate between a retrograde septal AP and AV nodal conduction in patients whose proximal CS recording shows no visible ventricular electrogram.
Keywords: Accessory pathway; Atrioventricular node; Para-Hisian pacing.
Figures


References
-
- Hirao K., Otomo K., Wang X. Para-Hisian pacing. A new method for differentiating retrograde conduction over an accessory AV pathway from conduction over the AV node. Circulation. 1996;94:1027–1035. - PubMed
-
- Nakagawa H., Jackman W.M. Para-Hisian pacing: useful clinical technique to differentiate retrograde conduction between accessory atrioventricular pathways and atrioventricular nodal pathways. Heart Rhythm. 2005;2:667–672. - PubMed
-
- Hirao K., Yamamoto N., Toshida N. Diagnostic significance of the morphological change in the atrial electrogram during para-Hisian pacing. Jpn Circ J. 2000;64:928–932. - PubMed
-
- Adachi M., Igawa O., Miake J. QRS complex widening due to loss of left bundle branch capture: pitfall of para-Hisian pacing. J Interv Card Electrophysiol. 2009;25:213–216. - PubMed
-
- van Opstal J.M., Crijns H.J. Paradoxical increase of stimulus to atrium interval despite His-bundle capture during para-Hisian pacing. Europace. 2009;11:1702–1704. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
