

Friedreich ataxia in Norway - an epidemiological, molecular and clinical study
- PMID: 26338206
- PMCID: PMC4559212
- DOI: 10.1186/s13023-015-0328-4
Friedreich ataxia in Norway - an epidemiological, molecular and clinical study
Abstract
Background: Friedreich ataxia is an autosomal recessive hereditary spinocerebellar disorder, characterized by progressive limb and gait ataxia due to proprioceptive loss, often complicated by cardiomyopathy, diabetes and skeletal deformities. Friedreich ataxia is the most common hereditary ataxia, with a reported prevalence of 1:20 000 - 1:50 000 in Central Europe. Previous reports from south Norway have found a prevalence varying from 1:100 000 - 1:1 350 000; no studies are previously done in the rest of the country.
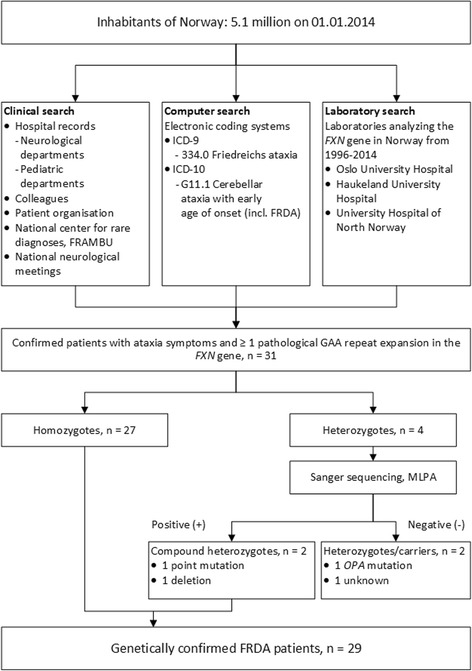
Methods: In this cross-sectional study, Friedreich ataxia patients were identified through colleagues in neurological, pediatric and genetic departments, hospital archives searches, patients' associations, and National Centre for Rare Disorders. All included patients, carriers and controls were investigated clinically and molecularly with genotype characterization including size determination of GAA repeat expansions and frataxin measurements. 1376 healthy blood donors were tested for GAA repeat expansion for carrier frequency analysis.
Results: Twenty-nine Friedreich ataxia patients were identified in Norway, of which 23 were ethnic Norwegian, corresponding to a prevalence of 1:176 000 and 1:191 000, respectively. The highest prevalence was seen in the north. Carrier frequency of 1:196 (95 % CI = [1:752-1:112]) was found. Homozygous GAA repeat expansions in the FXN gene were found in 27/29, while two patients were compound heterozygous with c.467 T < C, L157P and the deletion (g.120032_122808del) including exon 5a. Two additional patients were heterozygous for GAA repeat expansions only. Significant differences in the level of frataxin were found between the included patients (N = 27), carriers (N = 37) and controls (N = 27).
Conclusions: In this first thorough study of a complete national cohort of Friedreich ataxia patients, and first nation-wide study of Friedreich ataxia in Norway, the prevalence of Friedreich ataxia in Norway is lower than in Central Europe, but higher than in the last Norwegian report, and as expected from migration studies. A south-north prevalence gradient is present. Based on Hardy Weinberg's equilibrium, the carrier frequency of 1:196 is consistent with the observed prevalence. All genotypes, and typical and atypical phenotypes were present in the Norwegian population. The patients were phenotypically similar to European cohorts. Frataxin was useful in the diagnostic work-up of heterozygous symptomatic cases.
Figures



References
-
- Bidichandani SI, Delatycki MB. Friedreich Ataxia. Pagon R, Adam M, HH A, editors. Seattle, USA: University of Washington, Seattle; 1998 (Updated 2014 Jul 24). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
