

Variation in hospital rates of induction of labour: a population-based record linkage study
- PMID: 26338687
- PMCID: PMC4563219
- DOI: 10.1136/bmjopen-2015-008755
Variation in hospital rates of induction of labour: a population-based record linkage study
Abstract
Objectives: To examine interhospital variation in rates of induction of labour (IOL) to identify potential targets to reduce high rates of practice variation.
Design: Population-based record linkage cohort study.
Setting: New South Wales, Australia, 2010-2011.
Participants: All women with live births of ≥24 weeks gestation in 72 hospitals.
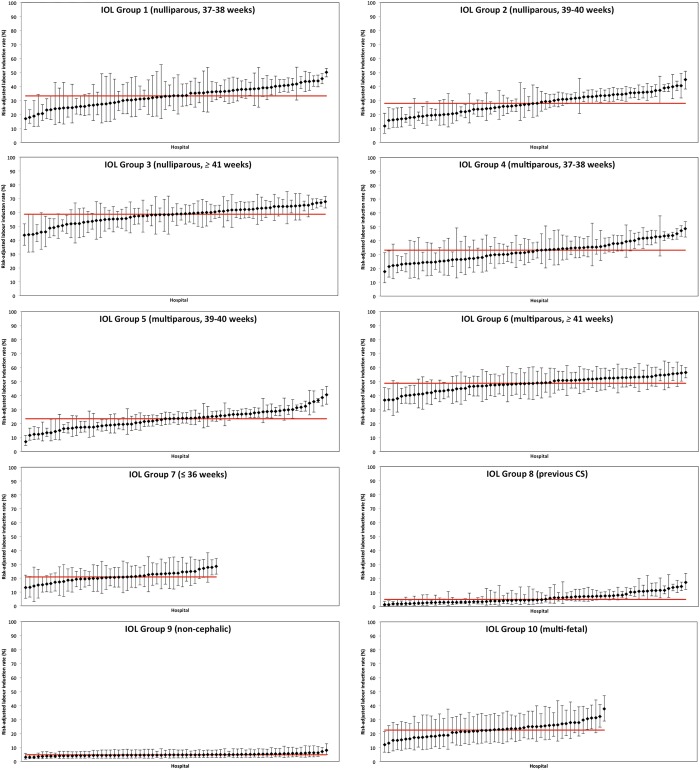
Primary outcome measure: Variation in hospital IOL rates adjusted for differences in case-mix, according to 10 mutually exclusive groups derived from the Robson caesarean section classification; groups were categorised by parity, plurality, fetal presentation, prior caesarean section and gestational age.
Results: The overall IOL rate was 26.7% (46,922 of 175,444 maternities were induced), ranging from 9.7% to 41.2% (IQR 21.8-29.8%) between hospitals. Nulliparous and multiparous women at 39-40 weeks gestation with a singleton cephalic birth were the greatest contributors to the overall IOL rate (23.5% and 20.2% of all IOL respectively), and had persisting high unexplained variation after adjustment for case-mix (adjusted hospital IOL rates ranging from 11.8% to 44.9% and 7.1% to 40.5%, respectively). In contrast, there was little variation in interhospital IOL rates among multiparous women with a singleton cephalic birth at ≥41 weeks gestation, women with singleton non-cephalic pregnancies and women with multifetal pregnancies.
Conclusions: 7 of the 10 groups showed high or moderate unexplained variation in interhospital IOL rates, most pronounced for women at 39-40 weeks gestation with a singleton cephalic birth. Outcomes associated with divergent practice require determination, which may guide strategies to reduce practice variation.
Keywords: EPIDEMIOLOGY; OBSTETRICS.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical