

Cerebral Angiography for Evaluation of Patients with CT Angiogram-Negative Subarachnoid Hemorrhage: An 11-Year Experience
- PMID: 26338924
- PMCID: PMC7959954
- DOI: 10.3174/ajnr.A4503
Cerebral Angiography for Evaluation of Patients with CT Angiogram-Negative Subarachnoid Hemorrhage: An 11-Year Experience
Abstract
Background and purpose: CT angiography is increasingly used to evaluate patients with nontraumatic subarachnoid hemorrhage given its high sensitivity for aneurysms. We investigated the yield of digital subtraction angiography among patients with SAH or intraventricular hemorrhage and a negative CTA.
Materials and methods: An 11-year, single-center retrospective review of all consecutive patients with CTA-negative SAH was performed. Noncontrast head CT, CTA, DSA, and MR imaging studies were reviewed by 2 experienced interventional neuroradiologists and 1 neuroradiologist.
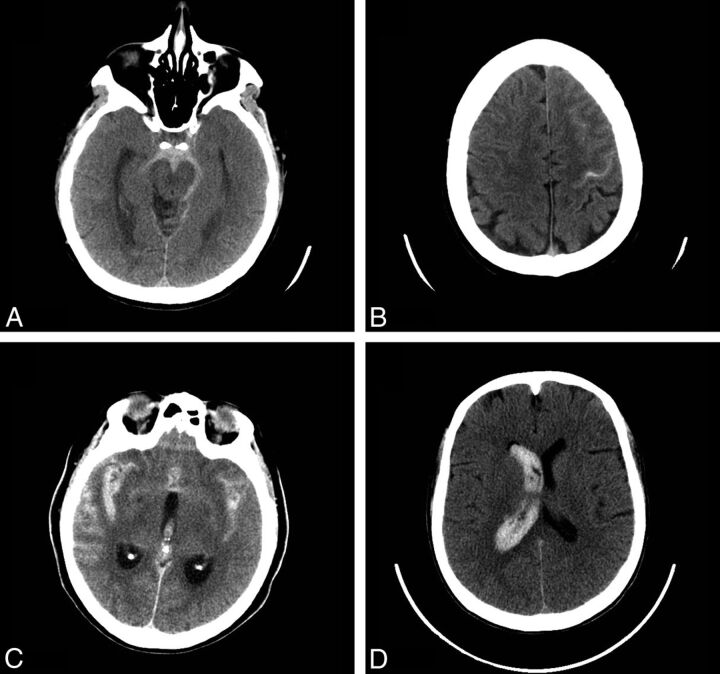
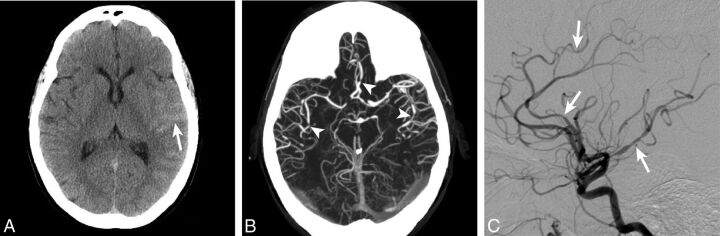
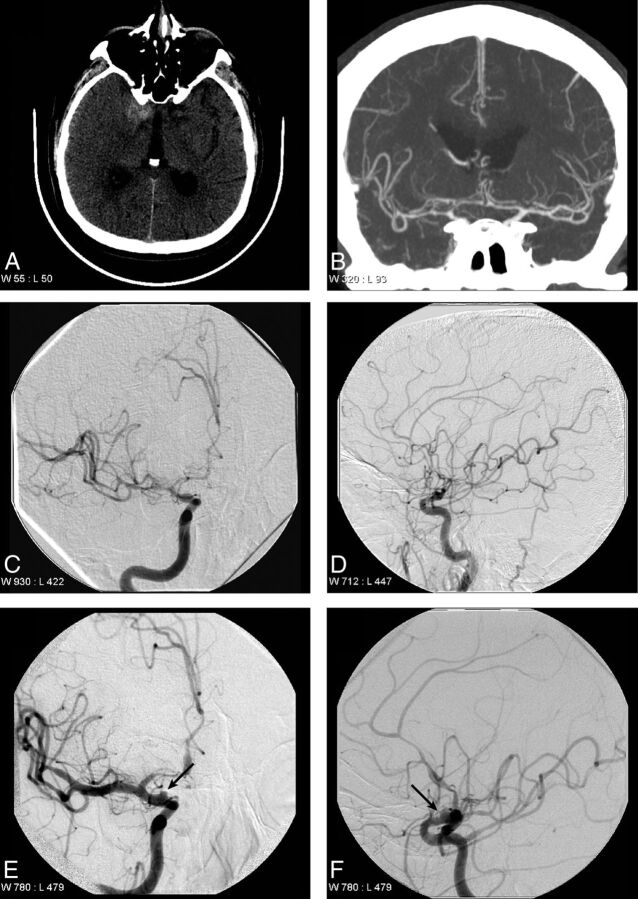
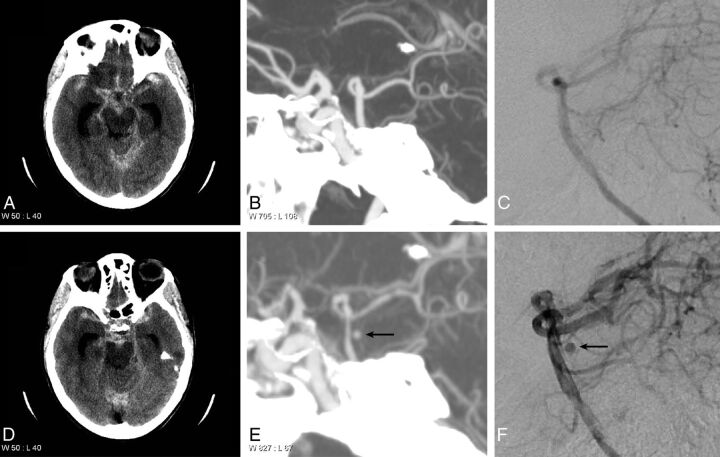
Results: Two hundred thirty patients (mean age, 54 years; 51% male) with CTA-negative SAH were identified. The pattern of SAH was diffuse (40%), perimesencephalic (31%), sulcal (31%), isolated IVH (6%), or identified by xanthochromia (7%). Initial DSA yield was 13%, including vasculitis/vasculopathy (7%), aneurysm (5%), arteriovenous malformation (0.5%), and dural arteriovenous fistula (0.5%). An additional 6 aneurysms/pseudoaneurysms (4%) were identified by follow-up DSA, and a single cavernous malformation (0.4%) was identified by MRI. No cause of hemorrhage was identified in any patient presenting with isolated intraventricular hemorrhage or xanthochromia. Diffuse SAH was due to aneurysm rupture (17%); perimesencephalic SAH was due to aneurysm rupture (3%) or vasculitis/vasculopathy (1.5%); and sulcal SAH was due to vasculitis/vasculopathy (32%), arteriovenous malformation (3%), or dural arteriovenous fistula (3%).
Conclusions: DSA identifies vascular pathology in 13% of patients with CTA-negative SAH. Aneurysms or pseudoaneurysms are identified in an additional 4% of patients by repeat DSA following an initially negative DSA. All patients with CT-negative SAH should be considered for DSA. The pattern of SAH may suggest the cause of hemorrhage, and aneurysms should specifically be sought with diffuse or perimesencephalic SAH.
© 2016 by American Journal of Neuroradiology.
Figures
Comment in
-
Reply.AJNR Am J Neuroradiol. 2016 Jun;37(6):E54. doi: 10.3174/ajnr.A4802. Epub 2016 Apr 7. AJNR Am J Neuroradiol. 2016. PMID: 27056429 Free PMC article. No abstract available.
-
Regarding "Cerebral Angiography for Evaluation of Patients with CT Angiogram-Negative Subarachnoid Hemorrhage: An 11-Year Experience".AJNR Am J Neuroradiol. 2016 Jun;37(6):E52-3. doi: 10.3174/ajnr.A4794. Epub 2016 Apr 7. AJNR Am J Neuroradiol. 2016. PMID: 27056430 Free PMC article. No abstract available.
References
-
- Bederson JB, Connolly ES Jr, Batjer HH, et al. ; American Heart Association. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 2009;40:994–1025 10.1161/STROKEAHA.108.191395 - DOI - PubMed
-
- Kaim A, Proske M, Kirsch E, et al. Value of repeat-angiography in cases of unexplained subarachnoid hemorrhage (SAH). Acta Neurol Scand 1996;93:366–73 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources