

Challenges in the Treatment of Chronic Wounds
- PMID: 26339534
- PMCID: PMC4528992
- DOI: 10.1089/wound.2015.0635
Challenges in the Treatment of Chronic Wounds
Abstract
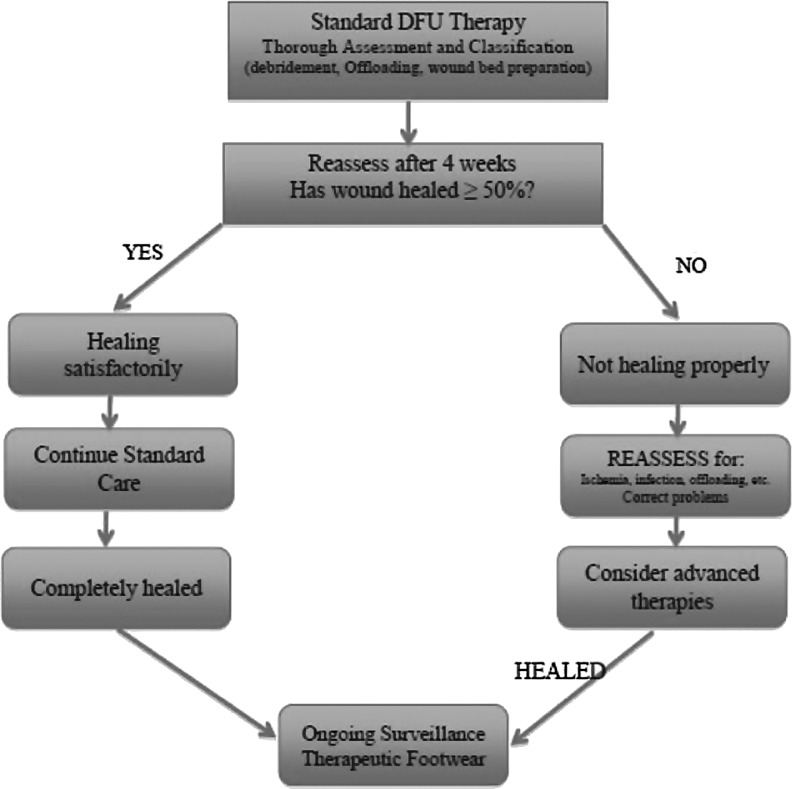
Significance: Chronic wounds include, but are not limited, to diabetic foot ulcers, venous leg ulcers, and pressure ulcers. They are a challenge to wound care professionals and consume a great deal of healthcare resources around the globe. This review discusses the pathophysiology of complex chronic wounds and the means and modalities currently available to achieve healing in such patients. Recent Advances: Although often difficult to treat, an understanding of the underlying pathophysiology and specific attention toward managing these perturbations can often lead to successful healing. Critical Issues: Overcoming the factors that contribute to delayed healing are key components of a comprehensive approach to wound care and present the primary challenges to the treatment of chronic wounds. When wounds fail to achieve sufficient healing after 4 weeks of standard care, reassessment of underlying pathology and consideration of the need for advanced therapeutic agents should be undertaken. However, selection of an appropriate therapy is often not evidence based. Future Directions: Basic tenets of care need to be routinely followed, and a systematic evaluation of patients and their wounds will also facilitate appropriate care. Underlying pathologies, which result in the failure of these wounds to heal, differ among various types of chronic wounds. A better understanding of the differences between various types of chronic wounds at the molecular and cellular levels should improve our treatment approaches, leading to better healing rates, and facilitate the development of new more effective therapies. More evidence for the efficacy of current and future advanced wound therapies is required for their appropriate use.
Figures
References
-
- Brownrigg JR, Apelqvist J, Bakker K, Schaper NC, Hinchliffe RJ. Evidence-based management of PAD & the diabetic foot. Eur J Vasc Endovasc Surg 2013;45:673–681 - PubMed
-
- Richmond NA, Maderal AD, Vivas AC. Evidence-based management of common chronic lower extremity ulcers. Dermatol Ther 2013;26:187–196 - PubMed
-
- Canadian Agency for Drugs and Technologies in Health. Optimal Care of Chronic, Non-Healing, Lower Extremity Wounds: A Review of Clinical Evidence and Guidelines. Ottawa, ON, Canada, 2013 - PubMed
-
- Rice JB, Desai U, Cummings AK, Birnbaum HG, Skornicki M, Parsons NB. Burden of diabetic foot ulcers for medicare and private insurers. Diabetes Care 2014;37:651–658 - PubMed
-
- Shankaran V, Brooks M, Mostow E. Advanced therapies for chronic wounds: NPWT, engineered skin, growth factors, extracellular matrices. Dermatol Ther 2013;26:215–221 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
