

Singapore Tele-technology Aided Rehabilitation in Stroke (STARS) trial: protocol of a randomized clinical trial on tele-rehabilitation for stroke patients
- PMID: 26341358
- PMCID: PMC4560876
- DOI: 10.1186/s12883-015-0420-3
Singapore Tele-technology Aided Rehabilitation in Stroke (STARS) trial: protocol of a randomized clinical trial on tele-rehabilitation for stroke patients
Abstract
Background: Most acute stroke patients with disabilities do not receive recommended rehabilitation following discharge to the community. Functional and social barriers are common reasons for non-adherence to post-discharge rehabilitation. Home rehabilitation is an alternative to centre-based rehabilitation but is costlier. Tele-rehabilitation is a possible solution, allowing for remote supervision of rehabilitation and eliminating access barriers. The objective of the Singapore Tele-technology Aided Rehabilitation in Stroke (STARS) trial is to determine if a novel tele-rehabilitation intervention for the first three months after stroke admission improves functional recovery compared to usual care.
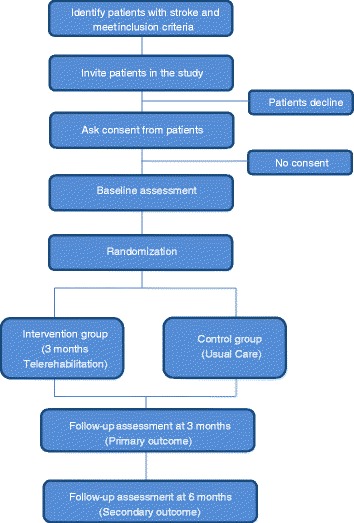
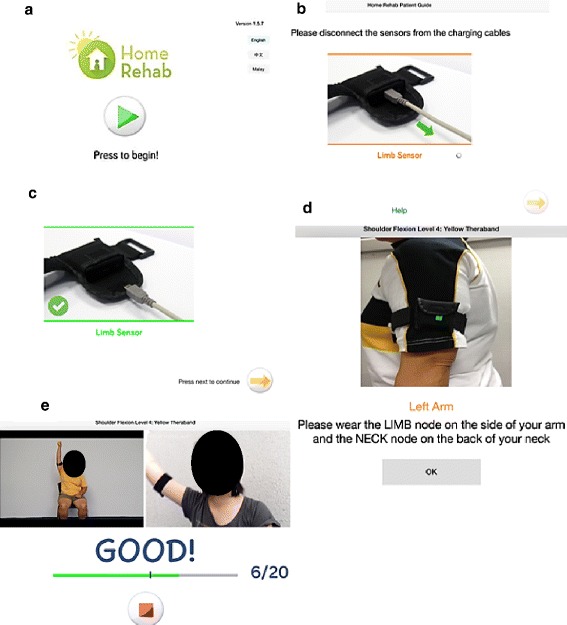
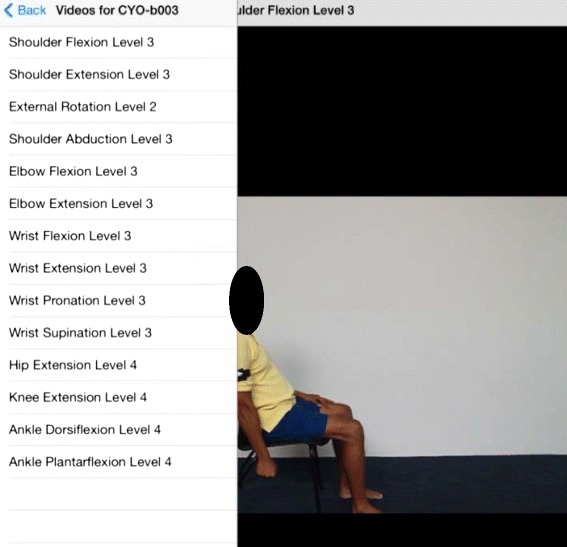
Methods/design: This is a single blind (evaluator blinded), parallel, two-arm randomised controlled trial study design involving 100 recent stroke patients. The inclusion criteria are age ≥40 years, having caregiver support and recent stroke defined as stroke diagnosis within 4 weeks. Consenting participants will be randomized with varying block size of 4 or 6 assuming a 1:1 treatment allocation with the participating centre as the stratification factor. The baseline assessment will be done within 4 weeks of stroke onset, followed by follow-up assessments at 3 and 6 months. The tele-rehabilitation intervention lasts for 3 months and includes exercise 5-days-a-week using an iPad-based system that allows recording of daily exercise with video and sensor data and weekly video-conferencing with tele-therapists after data review. Those allocated to the control group will receive usual care. The primary outcome measure is improvement in life task's social activity participation at three months as measured by the disability component of the Jette Late Life Functional and Disability Instrument (LLFDI). Secondary outcome variables consist of gait speed (Timed 5-Meter Walk Test) and endurance (Two-Minute Walk test), performance of basic activities of daily living (Shah-modified Barthel Index), balance confidence (Activities-Specific Balance Confidence Scale), patient self-reported health-related quality-of-life [Euro-QOL (EQ-5D)], health service utilization (Singapore Stroke Study Health Service Utilization Form) and caregiver reported stress (Zarit Caregiver Burden Inventory).
Discussion: The goal of this trial is to provide evidence on the potential benefit and cost-effectiveness of this novel tele-rehabilitation programme which will guide health care decision-making and potentially improve performance of post-stroke community-based rehabilitation.
Trial registration: This trial protocol was registered under ClinicalTrials.gov on 18 July 2013 as study title "The Singapore Tele-technology Aided Rehabilitation in Stroke (STARS) Study" (ID: The STARS Study, ClinicalTrials.gov Identifier: NCT01905917 ).
Figures
References
-
- Tangeman PT, Banaitis DA, Williams AK. Rehabilitation of chronic stroke patients: changes in functional performance. Arch Phys Med Rehabil. 1990;71:876–80. - PubMed
-
- Chen AW, Koh YT, Leong SW, Ng LW, Lee PS, Koh GC. Post Community Hospital Discharge Rehabilitation Attendance: Self-Perceived Barriers and Participation over Time. Ann Acad Med Singapore. 2014;43:136–44. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
