

Prognostic significance of tumor-infiltrating CD8+ and FOXP3+ lymphocytes in residual tumors and alterations in these parameters after neoadjuvant chemotherapy in triple-negative breast cancer: a retrospective multicenter study
- PMID: 26341640
- PMCID: PMC4560879
- DOI: 10.1186/s13058-015-0632-x
Prognostic significance of tumor-infiltrating CD8+ and FOXP3+ lymphocytes in residual tumors and alterations in these parameters after neoadjuvant chemotherapy in triple-negative breast cancer: a retrospective multicenter study
Abstract
Introduction: The status of tumor-infiltrating lymphocytes (TILs) has been recently proposed to predict clinical outcome of patients with breast cancer. We therefore studied the prognostic significance of CD8(+) TILs and FOXP3(+) TILs in residual tumors after neoadjuvant chemotherapy (NAC) and the alterations in these parameters before and after NAC in patients with triple-negative breast cancer (TNBC).
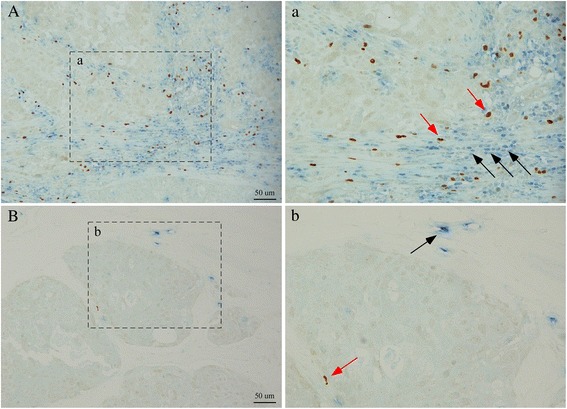
Methods: One hundred thirty-one TNBC patients who received NAC at three institutions were examined. CD8(+) TIL and FOXP3(+) TIL in residual tumors and biopsy specimens were evaluated by double-staining immunohistochemistry. The CD8(+) TIL and FOXP3(+) TIL status of the residual tumors was assessed, and the rates of their changes before and after NAC were calculated.
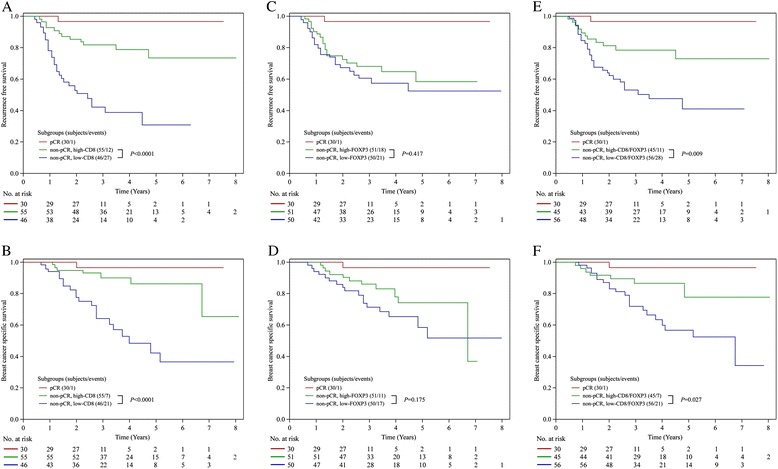
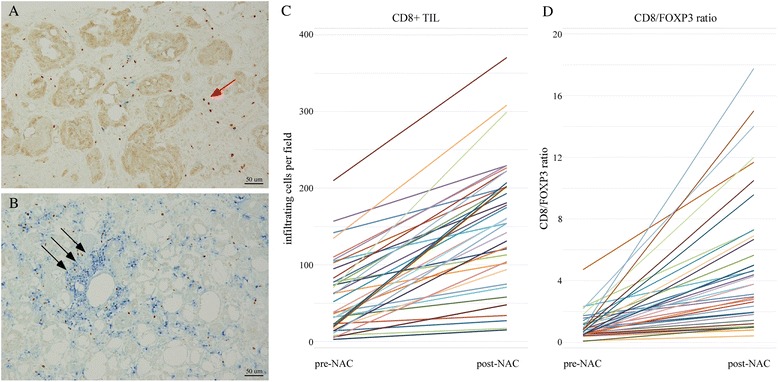
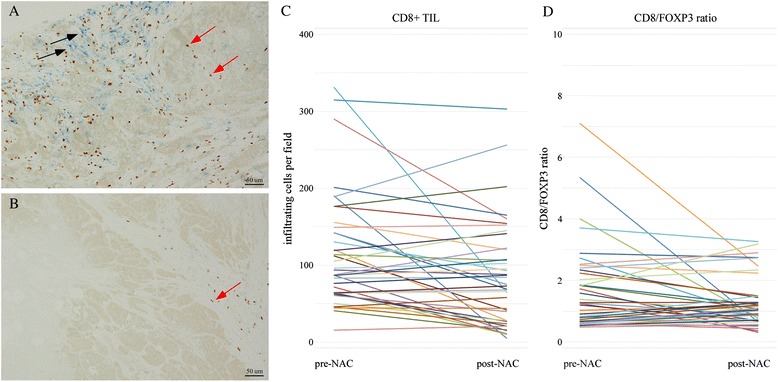
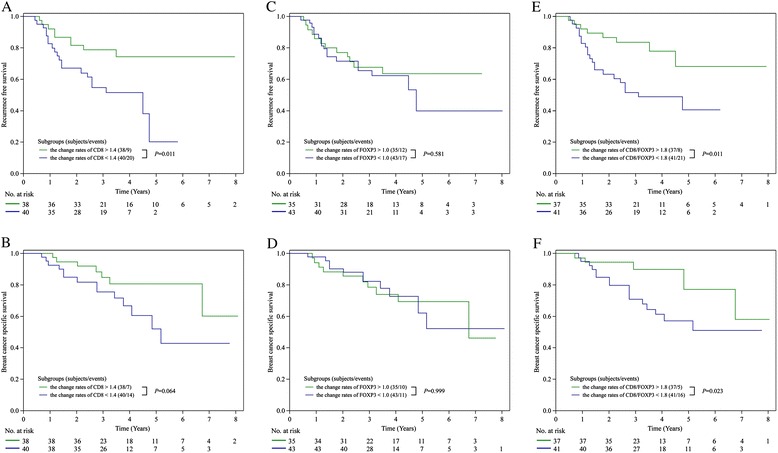
Results: TNBC patients with high CD8(+) TIL levels or a high CD8/FOXP3 ratio in residual tumors had significantly better recurrence-free survival (RFS) and breast cancer-specific survival (BCSS) than patients with low values of these parameters. In multivariate analyses, CD8(+) TIL exhibited strong prognostic significance for RFS, with a hazard ratio (HR) of 3.09 (95 % confidence interval (CI) 1.537-6.614, P=0.0013). The CD8/FOXP3 ratio was also significantly correlated with RFS (HR=2.07, 95 % CI 1.029-4.436, P=0.0412). TNBC with larger residual tumor size and positive lymph node status, which are known prognostic factors, was independently associated with worse RFS (P=0.0064 and P=0.0015, respectively). High CD8(+) TIL levels were a markedly powerful indicator of improved BCSS, with an HR of 3.59 (95 % CI 1.499-9.581, P=0.0036). Nodal status was also associated with BCSS (P=0.0024). TNBC with a high rate of CD8(+) TIL changes was associated with significantly better RFS compared with the low group (P=0.011). Higher rates of changes in the CD8/FOXP3 ratio were significantly correlated with both better RFS and BCSS compared with lower rates (P=0.011 and P=0.023, respectively).
Conclusions: This is the first study to demonstrate that high CD8(+) TIL and a high CD8/FOXP3 ratio in residual tumors and increment of these parameters following NAC and accurately predict improved prognosis in TNBC patients with non-pathological complete response following NAC. These parameters could serve as a surrogate one for adjuvant treatment in patients with residual disease in the neoadjuvant setting.
Figures
Similar articles
-
Prognostic implications of residual disease tumor-infiltrating lymphocytes and residual cancer burden in triple-negative breast cancer patients after neoadjuvant chemotherapy.Ann Oncol. 2019 Feb 1;30(2):236-242. doi: 10.1093/annonc/mdy547. Ann Oncol. 2019. PMID: 30590484
-
Tumor-infiltrating CD8+ and FOXP3+ lymphocytes in triple-negative breast cancer: its correlation with pathological complete response to neoadjuvant chemotherapy.Breast Cancer Res Treat. 2014 Dec;148(3):525-34. doi: 10.1007/s10549-014-3197-y. Epub 2014 Nov 14. Breast Cancer Res Treat. 2014. PMID: 25395319
-
Integration of tumour infiltrating lymphocytes, programmed cell-death ligand-1, CD8 and FOXP3 in prognostic models for triple-negative breast cancer: Analysis of 244 stage I-III patients treated with standard therapy.Eur J Cancer. 2020 Sep;136:7-15. doi: 10.1016/j.ejca.2020.05.014. Epub 2020 Jul 1. Eur J Cancer. 2020. PMID: 32622323
-
Prognostic value of tumor-infiltrating lymphocytes in patients with triple-negative breast cancer: a systematic review and meta-analysis.BMC Cancer. 2020 Mar 4;20(1):179. doi: 10.1186/s12885-020-6668-z. BMC Cancer. 2020. PMID: 32131780 Free PMC article.
-
The prognostic value of tumor-infiltrating lymphocytes in triple-negative breast cancer: a meta-analysis.Breast Cancer Res Treat. 2014 Dec;148(3):467-76. doi: 10.1007/s10549-014-3185-2. Epub 2014 Nov 1. Breast Cancer Res Treat. 2014. PMID: 25361613 Review.
Cited by
-
Rs-10889677 variant in interleukin-23 receptor may contribute to creating an inflammatory milieu more susceptible to bladder tumourigenesis: report and meta-analysis.Immunogenetics. 2021 Jun;73(3):207-226. doi: 10.1007/s00251-021-01205-w. Epub 2021 Mar 4. Immunogenetics. 2021. PMID: 33665735 Review.
-
Feasibility study on pre or postoperative accelerated radiotherapy (POP-ART) in breast cancer patients.Pilot Feasibility Stud. 2020 Oct 10;6:154. doi: 10.1186/s40814-020-00693-z. eCollection 2020. Pilot Feasibility Stud. 2020. PMID: 33062295 Free PMC article.
-
Prognostic Implications of the Residual Tumor Microenvironment after Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer Patients without Pathological Complete Response.Cancers (Basel). 2023 Jan 18;15(3):597. doi: 10.3390/cancers15030597. Cancers (Basel). 2023. PMID: 36765559 Free PMC article.
-
Regulation of chemo-sensitivity in ovarian cancer via a stroma dependent glutathione pathway.Transl Cancer Res. 2016 Sep;5(Suppl 3):S514-S519. doi: 10.21037/tcr.2016.09.32. Transl Cancer Res. 2016. PMID: 30542639 Free PMC article.
-
Microenvironment-derived ADAM28 prevents cancer dissemination.Oncotarget. 2018 Dec 14;9(98):37185-37199. doi: 10.18632/oncotarget.26449. eCollection 2018 Dec 14. Oncotarget. 2018. PMID: 30647853 Free PMC article.
References
-
- Caudle AS, Yu TK, Tucker SL, Bedrosian I, Litton JK, Gonzalez-Angulo AM, et al. Local-regional control according to surrogate markers of breast cancer subtypes and response to neoadjuvant chemotherapy in breast cancer patients undergoing breast conserving therapy. Breast Cancer Res. 2012;14:R83. doi: 10.1186/bcr3198. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
